multiple lymph nodes are involved, mediastinal masses in HD often appear elongated or lobulated in contour. Roughly spherical masses also can be seen (Fig. 5-5). Poor definition of the mass can indicate invasion or extension into adjacent lung.
TABLE 5.1 Hodgkin’s Disease | ||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||
 FIG. 5.1. HD involving superior mediastinal lymph nodes. A: PA chest radiograph shows bilateral lobulated superior mediastinal masses (arrows). B: The lateral view shows an anterior mediastinal mass (arrows). C: Contrast-enhanced CT scan shows prevascular anterior mediastinal lymph node enlargement (arrows) and pretracheal lymph node enlargement (*). Lymph node enlargement in these regions is typical of HD. |
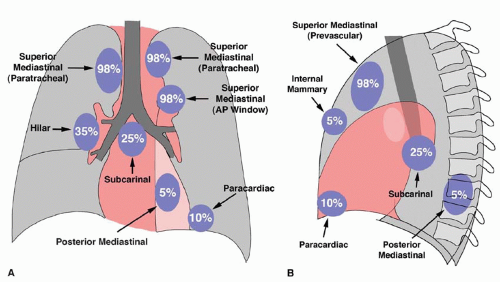 FIG. 5.2. Involvement of mediastinal lymph node groups in HD, illustrated as a percentage of patients with thoracic disease. Lymph node groups as shown on the PA (A) and lateral (B) radiographs. |
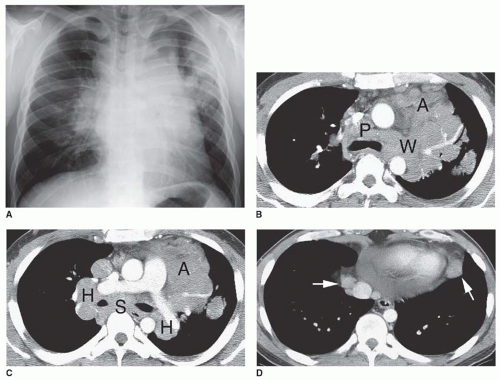 FIG. 5.3. HD with involvement of multiple lymph node groups. A: PA chest radiograph shows superior mediastinal widening, hilar enlargement, and nodules in the left upper lobe. B, C: Large lymph nodes are visible in the prevascular anterior mediastinum (A), pretracheal space (P), aortopulmonary window (W), subcarinal space (S), and both hila (H). Some discrete lymph nodes are visible, but other enlarged node masses appear matted together, with fat planes between them being invisible. D: Paracardiac lymph node enlargement (arrows) is visible at a lower level on CT. |
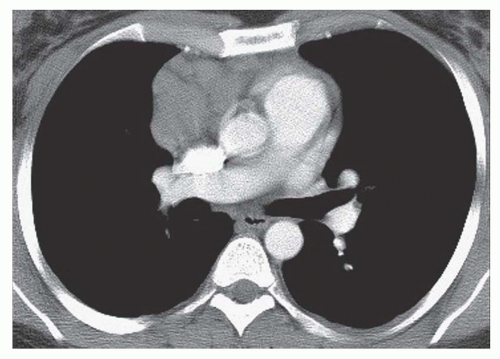 FIG. 5.4. Anterior mediastinal lymph node enlargement in nodular sclerosing HD. CT shows lymphadenopathy localized to the anterior mediastinum, which is typical of nodular sclerosing HD. |
intervening fat planes poorly seen; see Fig. 5-3B and C), or may be associated with diffuse mediastinal infiltration (with individual lymph nodes being invisible; see Fig. 5-5C and D). Most often, enlarged lymph nodes are of homogeneous soft tissue attenuation, but in 10% to 20% of cases, lymph node masses show areas of low attenuation or necrosis following contrast enhancement (Fig. 5-7). Inhomogeneity without obvious necrosis also may be seen (see Fig. 5-5D). Invasion of mediastinal structures such as the superior vena cava, esophagus, or airways may occur.
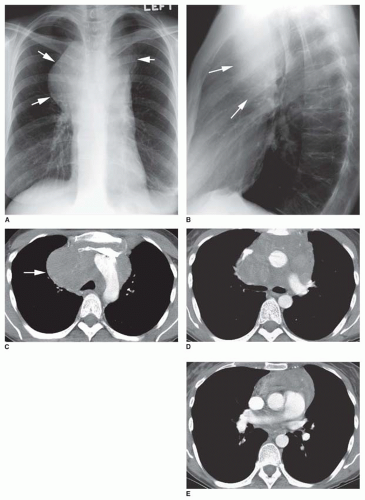 FIG. 5.5. Large mediastinal mass in HD. A: The PA radiograph shows a large spherical mass projecting to the right, with a smaller left-sided component (arrows). B: The lateral view shows the mass to be anterior (arrows). C: At the level of the aortic arch, CT shows a large, rounded mass that largely involves the pretracheal mediastinum (arrow). The opacified brachiocephalic veins are displaced anteriorly. Discrete nodal masses are not visible; the mediastinum appears infiltrated by tumor, and no mediastinal fat is visible. D: At the level of the left pulmonary artery, CT reveals that the mass occupies the prevascular anterior mediastinum and the precarinal space. The superior vena cava is displaced anteriorly and is compressed. At this level the mass appears somewhat inhomogenous in attenuation. Discrete, enlarged lymph nodes are not seen. E: At the level of the right pulmonary artery, anterior mediastinal mass appears to represent thymic involvement. |
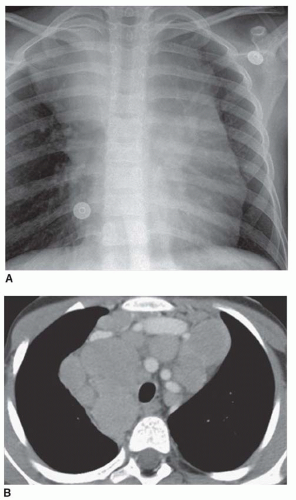 FIG. 5.6. HD in a 9-year-old child. A: Chest radiograph shows bilateral superior mediastinal masses. B: On CT, multiple discrete, enlarged lymph nodes are visible in the middle and anterior mediastinum. |
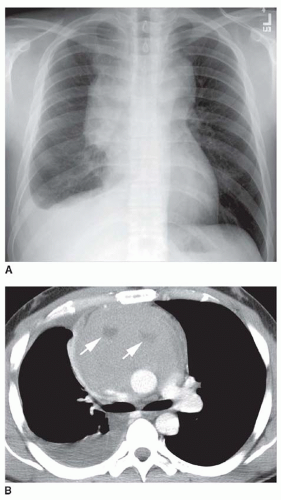 FIG. 5.7. Lymphoma with necrosis. A: Chest radiograph shows a large bilateral mediastinal mass and right pleural effusion, a portion of which is subpulmonic. B: Contrast-enhanced CT scan shows an anterior mediastinal mass containing an area of low attenuation (arrows). This finding is seen in 10% to 20% of patients with HD. |
 FIG. 5.8. Lymph node calcification following radiation treatment for HD. A: Coned-down lateral radiograph shows stippled calcification of enlarged anterior mediastinal lymph nodes (arrows), typical of radiated HD. Enlarged residual lymph nodes commonly are seen after treatment of HD. B, C: Focal calcifications of enlarged anterior mediastinal lymph nodes are shown on CT. Residual mediastinal lymph node masses following treatment of lymphoma are common, and most typical of nodular sclerosing HD. |
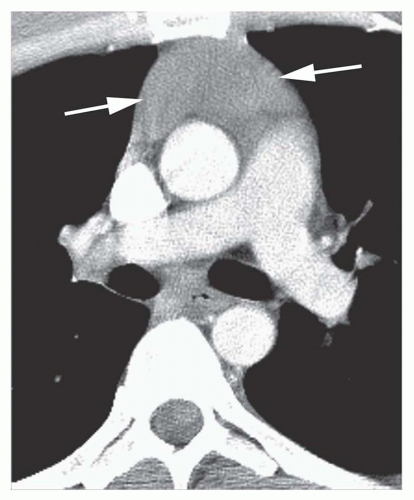 FIG. 5.9. Thymic involvement in HD. The thymus is enlarged but maintains a normal shape (arrows). |
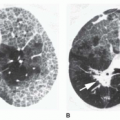
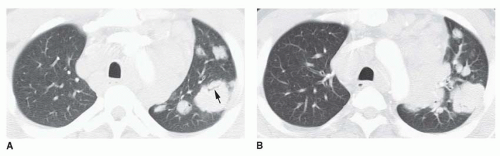 FIG. 5.10. Lung involvement in HD in the same patient shown in Figure 5-3. A, B: Large lobulated nodules are visible in the left lung. Some are associated with small bronchi or contain air bronchograms (arrow). Extensive mediastinal and hilar lymph node enlargement is present. |
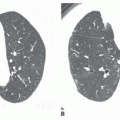
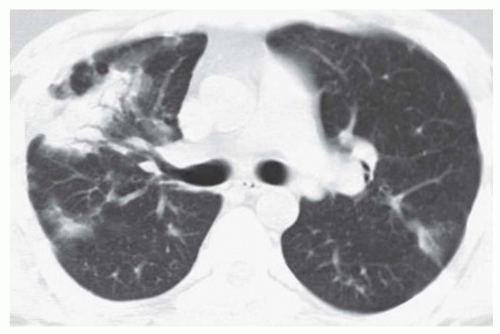 FIG. 5.11. Lung involvement in recurrent HD. Poorly defined nodules and areas of consolidation are visible. The large area of consolidation on the right contains a number of air bronchograms. There is no obvious lymph node enlargement. |
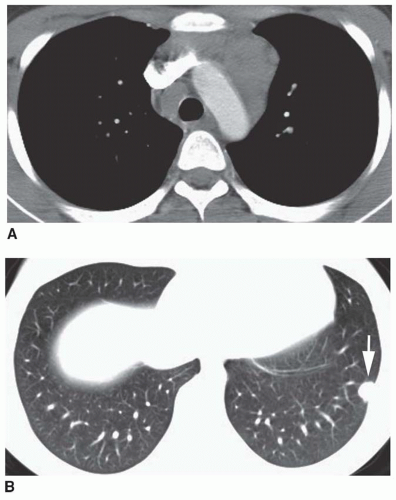 FIG. 5.12. Peripheral lung nodule in HD. A: CT shows pretracheal and prevascular lymph node enlargement. B: A small, well-defined subpleural nodule is visible in the left lung. This was found at biopsy to represent HD. |
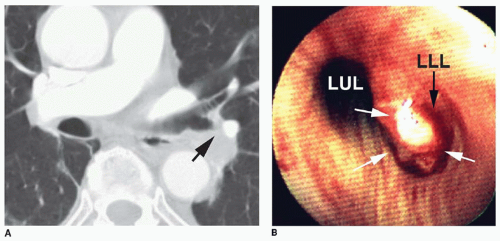 FIG. 5.13. Endobronchial HD. A: The left lower lobe bronchus is narrowed (arrow) by a polypoid endobronchial mass. B: Endoscopic photograph showing the left upper lobe bronchus (LUL) and a polypoid mass (white arrows) filling the left lower lobe bronchus (LLL). |
TABLE 5.2 Ann Arbor Staging Classification for Lymphoma | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||
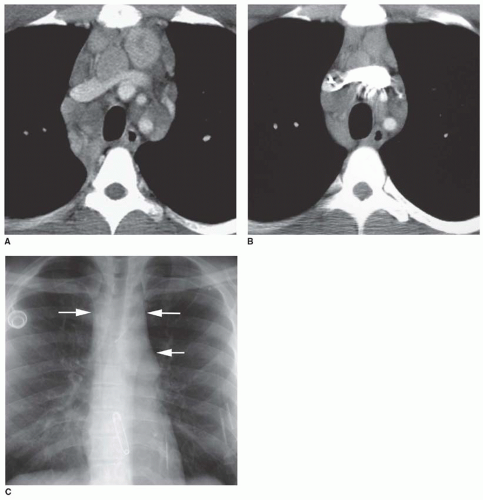 FIG. 5.14. Residual mediastinal mass in HD. A: CT scan before treatment shows multiple enlarged mediastinal lymph nodes. B: CT performed 2 years after treatment shows a decrease in lymph node size, but lymph nodes remain enlarged. Persistent enlarged lymph nodes are common after treatment of HD. C: Chest radiograph taken at the same time as the CT scan shown in (B) shows widening of the superior mediastinum and prominence of the aortopulmonary window (arrows). |
recurrence. Lymph node recurrence also may involve paracardiac lymph nodes, which usually are excluded from the treatment field because of their close relation to the heart (to avoid radiation pericarditis). Lung recurrence usually is associated with central or peripheral lung nodules, masses, or areas of focal consolidation, any of which may show cavitation. Lung recurrence is uncommonly associated with visible lymph node enlargement on chest radiographs, although it is visible on CT in about half of cases. Pleural effusions or masses and chest wall involvement also are common.
TABLE 5.3 Non-Hodgkin’s Lymphoma | ||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||
TABLE 5.4 Comparison of HD and NHL
Related posts:Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|
|---|