CHAPTER 105 Magnetic Resonance Imaging of Vascular Disorders of the Abdomen
INTRODUCTION
Gadolinium Agent Use and Safety
Concerns regarding the use of Gd-chelate contrast agents in the setting of renal disease have arisen since the initial description of a new disease, nephrogenic systemic fibrosis (NSF),1 and the subsequent correlation between prior Gd-chelate contrast agent exposure and development of NSF in patients with severe renal dysfunction.2 The current understanding of NSF is that nearly all cases have been attributed to exposure to gadodiamide (Omniscan) in more than 90% of peer-reviewed published cases, with the remainder of NSF cases associated with gadoversetamide (Optimark) or gadopentetate dimeglumine (Magnevist) exposure. Gadodiamide has relatively lower conditional stability, and it is believed that prolonged exposure to this agent, as occurs in the setting of reduced renal clearance, leads to greater chelate ligand dissociation and deposition of free gadolinium in tissues, including skin, leading to activation of the fibrotic process associated with NSF. NSF is primarily a disease affecting patients with severely impaired renal function (less than 15 mL/min) and mostly affecting patients on dialysis.1 Furthermore, NSF risk and severity appears to correlate with higher single and cumulative total gadodiamide dose.3 However, the risk of NSF using low dose, high relaxivity linear agents or high conditional stability cyclic agents appears immeasurably small; there remain no documented cases of NSF in the peer-reviewed literature with any of these other agents. Given concerns regarding NSF, we currently use a dose of 0.05 to 0.1 mmol/kg of a more stable high relaxivity linear or macrocyclic Gd-chelate contrast agent, mixed with an equal volume of normal saline. The contrast is then injected at a rate of 2 mL/s, followed by at least 20 mL of saline flush using a dual-chamber injector, which allows for a continuous influx of gadolinium during imaging. Our current understanding of NSF, and of contrast-induced nephropathy (CIN) associated with iodinated CT contrast, supports preferential use of contrast enhanced MRI over CT in patients with impaired renal function.4 Not yet published data documenting immeasurably low risk of higher cumulative dose administrations of high conditional stability cyclic agents may help to further define these dosage recommendations.
Cirrhosis and Portal Hypertension
Etiology and Pathophysiology
The parenchymal and vascular changes seen with MRI parallel the pathophysiologic changes occurring within the portal venous system, and are reflective of the underlying resistance to portal flow in the hepatic sinusoids. Chronic liver disease induces vasoconstriction within the hepatic microcirculation, owing to a relative lack of nitrous oxide (NO) and the action of potent vasoconstrictors.5 The larger portal venous branches dilate in a compensatory effort to increase portal flow. The reduction in NO within the hepatic microcirculation is reversed in the splanchnic vasculature,5 which also dilates in an attempt to increase portal flow and overcome developing resistance. An enlarged portal vein, superior mesenteric vein (SMV), and splenic vein are clear indicators of portal hypertension (Fig. 105-1). Flow in the portal vein, normally directed into the liver (hepatopetal) eventually reverses direction away from the liver (hepatofugal). These altered flow dynamics are most commonly assessed with ultrasound, although MRI has the capability to provide additional functional measures of portal flow that better correlate with the severity of cirrhosis and portal hypertension when compared with ultrasound.6 Continued increased resistance to portal flow in the hepatic sinusoids results in shunting of portal blood to the systemic venous system at predictable locations. Shunted blood pools at these sites of portosystemic anastomosis, causing the formation of varices.
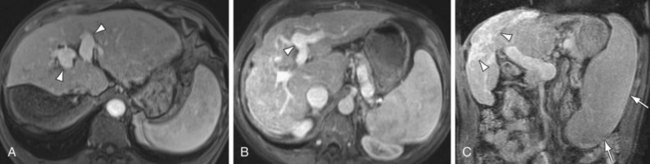
 FIGURE 105-1
FIGURE 105-1Manifestations of Disease
Imaging Indications and Algorithm
MRI has the unique ability to characterize underlying hepatic parenchymal changes prior to the development of frank portal hypertension. The hepatic fibrosis caused by repeated liver injury is seen on delayed phase, 3D GRE images, showing a fine or coarse reticular pattern of enhancement in the underlying hepatic parenchyma (Fig. 105-2). This reticular parenchymal enhancement can identify fibrotic liver disease before morphologic changes of cirrhosis and portal hypertension develop. This is a powerful tool in that it allows for an earlier, more aggressive treatment plan in patients at high risk for chronic liver disease. Conventional catheter angiography assesses strictly vascular morphology, which only typically becomes abnormal with more advanced disease and cannot evaluate parenchymal changes of fibrosis. CTA can also provide a noninvasive method of evaluating both vessels and soft tissues; however, it lacks the underlying contrast resolution to adequately assess fibrotic changes in the hepatic parenchyma. In addition, CTA and catheter angiography employ the use of ionizing radiation, a concern especially in the setting of chronic liver disease, which often requires repeated, multiphase imaging. MR is the only modality with the contrast and spatial resolution to fully assess the vasculature and hepatic parenchyma, with the added benefit of not employing ionizing radiation. Currently, early detection of fibrotic liver disease is primarily diagnosed through biopsy, but the use of MR to grade liver fibrosis may reduce the need for liver biopsy, which carries risks of hepatic injury, bleeding, and infection.
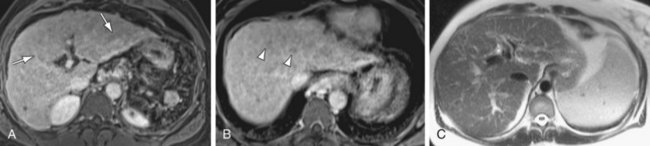
 FIGURE 105-2
FIGURE 105-2Imaging Techniques and Findings
MR
The most dangerous consequence of portosystemic shunting is bleeding from esophageal varices (Fig. 105-3). Varices may be identified within the esophageal wall (termed esophageal varices) or surrounding the esophagus (termed paraesophageal varices), although both drain the portal system via the left gastric (cardinal) vein. Additional common sites of variceal formation within the abdomen due to portosystemic shunting include gastric and retroperitoneal varices, spontaneous splenorenal shunts, and recanalized paraumbilical veins. Recanalized paraumbilical veins drain into the epigastric veins along the undersurface of the abdominal wall, often forming a mesh of dilated varices surrounding the umbilicus termed caput medusa (Fig. 105-4). Identification of paraumbilical varices are important in that the draining meshwork of superficial veins along the anterior abdominal wall must be avoided during diagnostic and therapeutic paracenteses that are often performed in patients with chronic liver disease. Although less common, intrahepatic portosystemic (venovenous shunts) may also occur in the setting of chronic liver disease as a result of increased portal resistance. These shunts have been described at the microscopic level7 and can also be identified with MR (Fig. 105-5). Other etiologies of intrahepatic portosystemic shunting include congenital malformations and rupture of a portal vein aneurysm into a hepatic vein, whereas post-traumatic shunts are most often associated with surgical interventions such as transhepatic catheter placement.
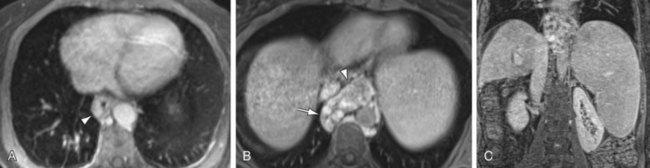
 FIGURE 105-3
FIGURE 105-3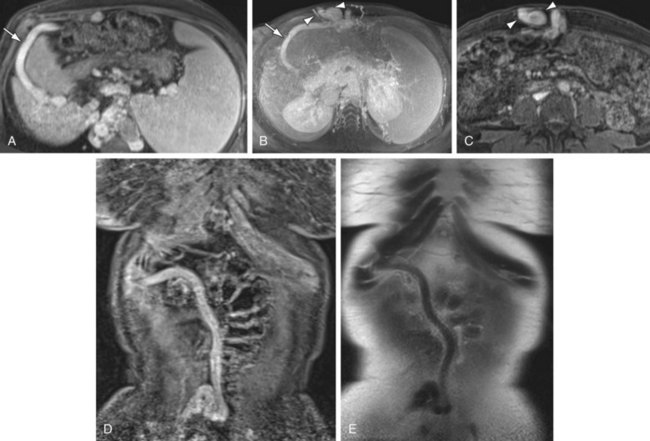
 FIGURE 105-4
FIGURE 105-4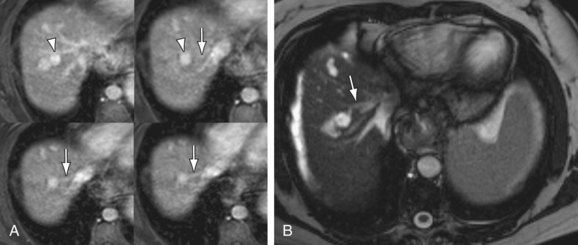
 FIGURE 105-5
FIGURE 105-5In addition to portosystemic shunting, chronic liver injury and fibrosis also causes arterioportal shunting, either secondary to underlying tumor (hepatocellular carcinoma) or cased by the parenchymal changes of fibrosis itself. These arterioportal shunts manifest on MR as small, linear- or wedge-shaped blushes of enhancement on arterial phase imaging, most often located along a capsular surface (Fig. 105-6). These foci of enhancement may be mistaken for a small tumor on CT owing to a relative lack of contrast resolution. However, MRI can more easily differentiate these small arterioportal shunts (APS) from hepatocellular carcinoma (HCC) in the majority of cases because the APS will show a more linear- or wedge-shaped morphology and will not demonstrate the washout and rim enhancement typical of HCC. Arterioportal shunts may also occur in settings other than chronic liver disease, such as trauma, iatrogenic (postbiopsy or surgery), congenital anomalies, or aneurysm rupture.8 APS are associated with both benign (hemangiomas) and malignant (HCC) hepatic tumors.9 APS also contribute to the flow changes seen in portal hypertension. Studies examining flow characteristics in the portal vein with intermittent occlusion of the hepatic artery have demonstrated that APS are a factor in hepatofugal flow of the portal vein in the setting of chronic liver disease.10
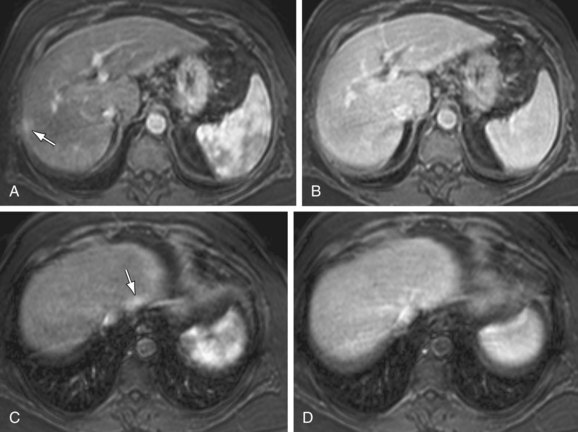
 FIGURE 105-6
FIGURE 105-6


Portal and Mesenteric Thrombosis
Imaging Techniques and Findings
MR
Intraluminal thrombus within the SMV is well demonstrated on MRI with 3D GRE images, providing a noninvasive method for diagnosis (Fig. 105-7). In addition, evaluation of the end-organ effects of mesenteric occlusion is important because the clinical picture varies between acute and chronic presentations, and not all patients require surgery. Bowel pathology can be evaluated concurrently with the vasculature using MRI, with ischemia demonstrating increased signal on fat-saturated T2W images secondary to inflammation and edema caused by venous congestion. The presence of bowel ischemia as identified by MR may prompt more aggressive therapy, with both percutaneous and intraoperative catheter-directed therapy demonstrating good results.11 Thrombosis of the splenic vein is a cause of isolated gastric varices and has been treated with splenectomy in the past, although percutaneous therapy has also been successful.
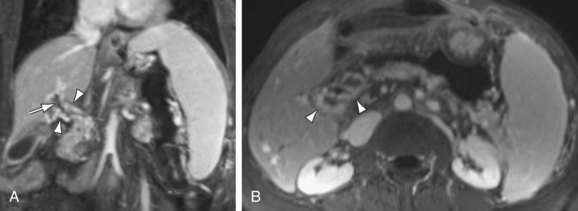
 FIGURE 105-7
FIGURE 105-7Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


