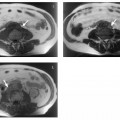
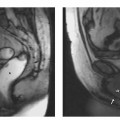
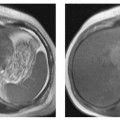
14 Magnetic Resonance Pelvimetry The aim of pelvimetry is to objectively measure pelvic dimensions and assess the configuration of the maternal bony pelvis to help obstetricians recognize fetopelvic disproportion and identify women who should have a primary cesarean section rather than attempt vaginal delivery. Ultrasound is the standard imaging modality for determining the weight and size of an unborn child. Conventional pelvimetry was a routine examination until the end of the 1950s. The number of pelvimetries rapidly declined with an increasing awareness of the risks of intrauterine radiation exposure and reports on the cancer risk associated with the examination.1,2 New techniques such as digital image enhancement radiography and CT have considerably reduced radiation exposure and led to a revival of maternal pelvic measurement. The use of MRI for pelvimetry was first described in 1985, and it has since evolved into the standard modality.2,3 MR pelvimetry is a highly accurate method, having a measurement error of only 1 %.3 Both fetal ultrasound and MR pelvimetry have very low interobserver and intraobserver variability.2,4 Different obstetric indices are determined to identify fetopelvic disproportion, but their use has increasingly come into question as they are limited in predicting the course of labor.1,2,5,6 As a consequence, the use of pelvimetry has shifted from the prenatal to the postnatal period to rule out a small pelvis in women with a history of protracted labor.1 It was shown that pelvimetry significantly reduces the rate of secondary cesarean sections in breech presentation (its most common indication).5 Performing an MRI examination during the first trimester (organogenesis) is generally discouraged.7–9 A deleterious effect on the fetus is not known; however, potential effects of the static magnetic field, the gradient system, and the high-frequency field used in MRI have not been investigated systematically.8 For this reason, the specific absorption rate (SAR) should be as low as possible. Although both GRE and SE sequences are considered harmless, the SAR of an SE or TSE sequence is several times higher than that of a GRE sequence, while both yield the same diagnostic image quality.6 MR pelvimetry not only obviates the need for exposure to ionizing radiation but also has several additional advantages: Despite its limited predictive value, there is a role for MR pelvimetry in the evaluation of the maternal pelvis. The radiologist’s task is to carry out the examination and measurement, while it is left to the experienced obstetrician to judge the clinical relevance of the findings. There is no generally accepted set of indications for MR pelvimetry. The importance attached to pelvimetry is at the discretion of the individual obstetrician and reflects the fact that the dimensions of the bony pelvis are only one of many factors that can lead to protracted labor. MR pelvimetry may be justified in the following situations:
M.R. Muehler
Introduction
Indications
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


