Abstract
The testes may demonstrate physiologic FDG avidity. Uncertain imaging findings in the testis on FDG PET/CT can be further evaluated with testicular ultrasound. FDG-avid foci within the prostate may represent benign focal prostatitis or prostate cancer. If needed, prostate MR could be used for further evaluation. Biopsy may be needed if a new diagnosis of prostate cancer would be clinically relevant.
Keywords
FDG, PET/CT, prostate, testes, prostate cancer, testicular cancer, orchitis
The male pelvis on 18F-fluorodeoxyglucose positron emission tomography/computed tomography (FDG PET/CT) is more straightforward than the female pelvis. The testes may demonstrate physiologic FDG avidity. FDG-avid foci within the prostate may represent benign focal prostatitis or prostate cancer.
Testes
Physiologic FDG Avidity in the Testes
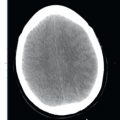
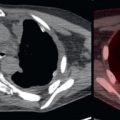
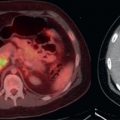
Physiologic FDG avidity is common in the testes ( Fig. 20.1 ). There is debate over how high a testicular standardized uptake value (SUV) may be and still be considered “physiologic.” If the testes are not enlarged on CT and there are no focal masses or FDG avidity in the testes, the FDG avidity is almost certainly physiologic. The testes are usually located within the scrotum; however, a testis may be located within the inguinal canal ( Fig. 20.2 ), which could lead to confusion with the inguinal lymph node. In young men with pelvic malignancy, beware of surgically transposed testes with physiologic FDG avidity in unexpected locations. If radiation is planned for the pelvis, the testes may be surgically transposed to remove them from the radiation port, to preserve their function and fertility ( Fig. 20.3 ).



Testicular Malignancies
Primary testicular malignancies include seminomas and nonseminomas. Testicular cancers may demonstrate lymphatic spread to lymph nodes. The gonadal lymphatics follow the testicular veins to the retroperitoneum; thus nodal metastases in the retroperitoneum may be apparent before lower pelvic nodal metastases. Alternatively, nodal metastases may be seen in the pelvis in the external iliac nodes. Internal iliac and inguinal nodes are normally not involved. Hematogenous spread to multiple organ systems, most commonly the lungs, may also occur.
The imaging technique of choice for visualizing and local staging of a primary testicular malignancy is ultrasound. There is no known clinically relevant role for FDG PET/CT in the T staging of testicular cancer. The imaging technique of choice for visualization and staging of nodal and distant metastases from testicular cancer is contrast-enhanced CT. FDG PET/CT may complement contrast-enhanced CT by detection of unsuspected FDG-avid metastases, such as nodal metastases or implants which are subcentimeter in size and thus overlooked on anatomic imaging.
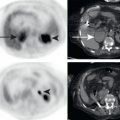
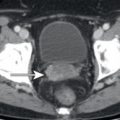
The testes may be sites of involvement by lymphoma or metastases. Physiologic FDG avidity in the testes is normally homogenous, and focal areas of increased FDG avidity are suspicious for disease involvement ( Fig. 20.4 ). In questionable cases, testicular ultrasound could be obtained for further evaluation.