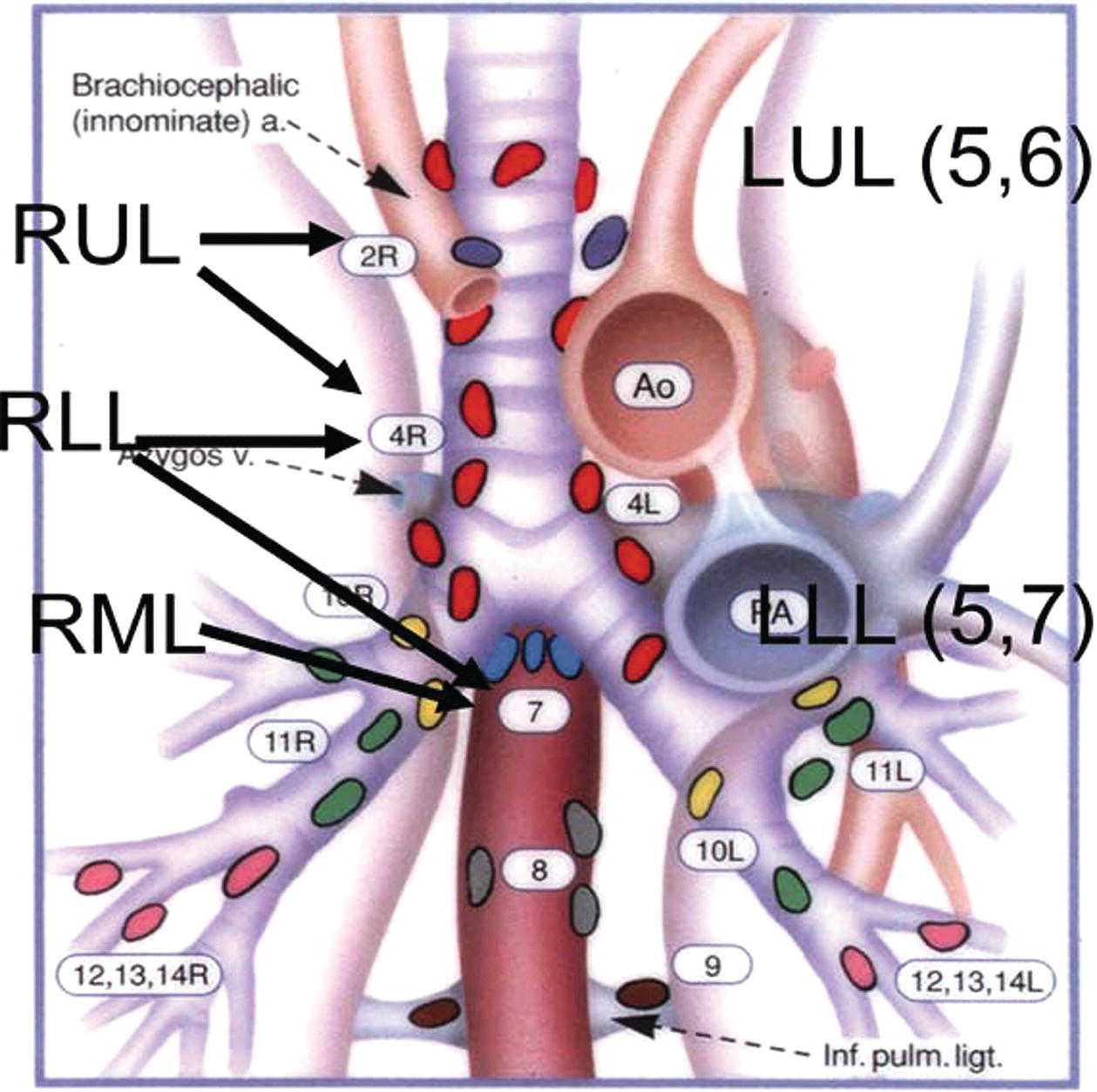
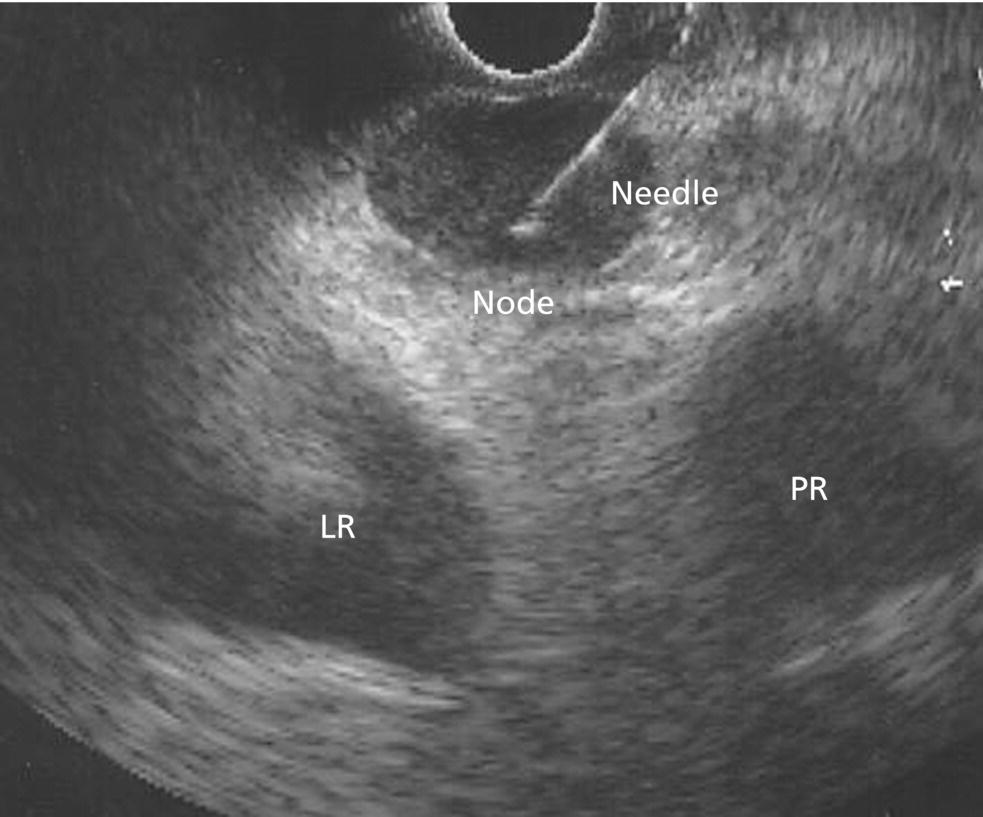
M. Babitha Reddy1, David H. Robbins1, and Mohamad A. Eloubeidi2 1 Lenox Hill Hospital, New York, NY, USA 2 American University of Beirut School of Medicine, Beirut, Lebanon Transesophageal endoscopic ultrasound (EUS) allows imaging of posterior mediastinal lymph nodes, which is where lung cancer as well as other cancers can metastasize. Additionally, large lung tumors abutting the esophagus can be imaged, as can primary posterior mediastinal lung tumors. EUS‐guided biopsies can be performed with either transesophageal endoscopic ultrasound‐guided fine needle aspiration (EUS‐FNA) or endobronchial ultrasound‐guided fine needle aspiration (EBUS‐FNA). The EUS characteristics of malignant lymph nodes include short axis diameter greater than 10 mm, round shape, well demarcated, and hypoechoic echotexture. Malignant mediastinal masses are generally greater than 3 cm in short axis diameter. Staging of lung cancer is based on the American Thoracic Society lymph node map (Figure 11.1). Transesophageal EUS can visualize the paratracheal lymph nodes (station 2), posterior aorto‐pulmonic window lymph nodes (station 5), subcarinal lymph nodes (station 7), and paraesophageal lymph nodes (station 8). In addition, transesophageal EUS can visualize other sites of metastases such as the left adrenal and the liver. EBUS can visualize stations 1, 2, 3, 4, 7, 10, and 11. Using a combination of both, nearly the entire posterior mediastinum can be visualized and biopsied, which obviates the need in most cases for diagnostic surgical mediastinoscopy. Figure 11.1 American Thoracic Society staging diagram for posterior mediastinal lymph nodes. Note that station 2 is paratracheal lymph nodes, station 5 is aorto‐pulmonic window, station 7 is subcarinal, and station 8 is paraesophageal. The superimposed lung locations show the lymphatic drainage of each part of the lung. LLL, left lower lobe; LUL, left upper lobe; RLL, right lower lobe; RML, right middle lobe; RUL, right upper lobe. Figure 11.2 Metastatic posterior mediastinal melanoma. Endoscopic ultrasound‐guided fine needle aspiration (EUS‐FNA) along with immunostains confirmed recurrent metastatic melanoma in the mediastinum. Figure 11.3 Renal cell cancer metastasis. The lesion was identified slightly above the gastroesophageal junction. Endoscopic ultrasound (EUS) was the only non‐surgical approach to reach this lesion. Intrapulmonary lung cancer drains to lymphadenopathy at various EUS and EBUS stations depending on the location of the cancer (Figure 11.1). The right upper lobe drains into stations 2R and 4R, accessible by EBUS. The right lower lobe drains into stations 4R and 7 accessible by EBUS and EUS, respectively. The right middle lobe drains into station 7 which is accessible by EBUS and EUS. Recent case series demonstrated safety in sampling lymph nodes and intrapulmonary masses at station 6, lateral to the aorta, via the trans‐aortic approach. The left upper lobe drains into stations 5 and 6 accessible by EUS and the left lower lobe drains into stations 5 and 7 accessible by EUS and EBUS (Figures 11.2–11.5). Figure 11.4 Lung cancer mass. Endoscopic ultrasound‐guided fine needle aspiration (EUS‐FNA) of a centrally located mass confirmed primary non‐small cell lung cancer. Figure 11.5 Malignant lymph node. The needle is within the rounded, well‐demarcated, hypoechoic lymph node. LA, left atrium; PA, pulmonary artery.
11
Malignant Mediastinal Lesions



Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


