Chapter 115
Medullary Thyroid Carcinoma
Epidemiology
Medullary carcinoma of the thyroid gland (MTC) is an uncommon malignancy and accounts for 5 to 10% of thyroid neoplasms. It occurs in either a sporadic or a familial form. The sporadic form accounts for 70% of cases and is primarily a tumor of middle-aged adults with a female to male ratio of 1.3:1. The familial form is inherited in an autosomal dominant pattern and expressed clinically as multiple endocrine neoplasia (MEN), types IIa and IIb, or as familial MTC alone (10–20%). The tumor is slightly more common in females and is seen in children as well as adults.
Clinical Findings
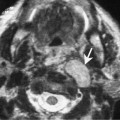
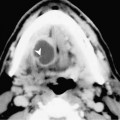
Patients generally present with a lower neck mass. Sipple’s syndrome (MEN IIa) is the association of medullary carcinoma with pheochromocytoma and parathyroid adenomas/hyperplasia. MEN IIb is said to be present when mucosal neuromas and marfanoid facies coexist with medullary thyroid carcinoma.
Pathology
MTC arises from the parafollicular C cells of the thyroid gland. MTC cells secrete the poly-peptide hormone calcitonin that serves as a tumor marker. The ‘ret’ protooncogene is consistently expressed in cases of MEN IIa. On gross examination, the tumor is soft to firm and well circumscribed but not encapsulated. Familial and sporadic variants are indistinguishable histologically. Individual tumor cells may be round, polygonal, or spindle-shaped and show eccentric nuclei with eosinophilic cytoplasm. Foci of necrosis and hemorrhage may be seen. Amyloid deposits are present in almost 50% of cases.
Treatment