CHAPTER 43 Meningioma
Epidemiology
Meningioma is a benign neoplasm arising from the arachnoid cap cells in the internal auditory canal-cerebellopontine angle (IAC-CPA) cistern. These lesions account for approximately 15 to 18% of all primary intracranial tumors; 10% occur in the posterior fossa, 10% are multiple, and meningiomas along with schwannomas commonly occur in patients with neurofibromatosis-2 (NF2). Meningiomas are the second most common CPA-IAC tumor encountered after vestibular schwannoma and second most common primary intracranial tumor. Meningiomas are more common in females.
Clinical Features
These lesions are often incidentally detected, as patients are usually asymptomatic. If present, the symptoms are caused by compression of adjacent neural structures. Thus the patients may present with hearing loss, tinnitus, headache, or signs and symptoms related to trigeminal nerve. These lesions are common in the middle-aged and the elderly, with peak age of incidence being 60 years. When associated with NF2, they may be seen in children.
Pathology
Meningiomas arise from the arachnoid cap cells and not from the dura. These tumors are sharply circumscribed and unencapsulated. Approximately 60% of sporadic meningiomas are caused by in-activation of the NF2 tumor suppressor gene on chromosome 22. No causative genetic abnormality is known for the remaining 40%. Angiogenic factors such as fibroblast growth factor-2 (FGF-2), vascular endothelial growth factor (VEGF), and integrins are expressed in meningiomas. Meningiomas have also been found to have receptors to many hormones such as progesterone and prolactin and may express growth hormone.
The 2000 World Health Organization (WHO) classification grades meningiomas as benign (grade I), atypical (grade II), and anaplastic (grade III). There is a wide range of histologic subtypes with little bearing on prognostic outcome. These include those that have lobules of meningothelial cells; fibrous type with parallel, interlacing fascicles of spindle shaped cells; transitional with mixed type, which are characterized by onion bulb whorls and lobules; psammomatous type, which contains numerous small calcifications; and angiomatous comprising abundant vascular channels. There are miscellaneous forms that include microcystic, secretory, lymphoplasmocyte-rich meningioma, chondroid, clear cell, atypical, papillary, anaplastic, and rhabdoid meningiomas.
Treatment
Surgical resection is the treatment of choice. Radiotherapy may be used as adjuvant or as primary treatment if the lesions invade adjacent eloquent neurovascular structures.
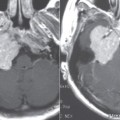
Imaging Findings
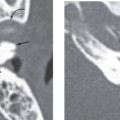
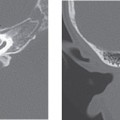
CT



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


