The Erlenmeyer flask shape describes the distal femur when the metaphysis is broad and the transition zone of the diaphysis is wide (Fig. 5.67). The Erlenmeyer flask shape is always the result of a pathologic process: either failure of remodeling (bone dysplasia) or expansion of the marrow space (infiltrative processes).
Fig. 5.67 Osteopetrosis. Erlenmeyer flask deformity in a patient with osteopetrosis.
Table 5.41 Metaphysis: broad metaphysis without cupping (Erlenmeyer flask)
Diagnosis
Findings
Comments
Fibrous dysplasia
Well-demarked lucent lesion with ground-glass matrix and cortical thinning in areas of expansion.
Bowing of the affected bones is common (shepherd’s crook in the proximal femur). Most lesions are located in the diaphysis. McCune-Albright syndrome: polyostotic fibrous dysplasia, skin pigmentation, and endocrinopathies (precocious puberty).
Thalassemia major
Coarse trabecular pattern. The medulla is expanded, causing cortical thinning.
Marrow infiltration from increased red marrow.
Sickle cell anemia (homozygous)
Similar appearance as thalassemia except for bone infarcts and AVN.
The marrow hyperplasia is milder in the heterozygous form, thus without the Erlenmeyer flask deformity.
Healing rickets
Erlenmeyer flask deformity seen during the healing phase.
Healing with periosteal new bone formation may extend into the diaphysis.
Normal width of the native metaphysis may sometimes be discerned within the periosteal new bone of the healing fracture. Follows metaphyseal fracture of infancy (child abuse, osteogenesis imperfecta).
Chronic lead and bismuth toxicity
Dense transverse metaphyseal band.
Gaucher disease
Symmetric and marked widening of the distal femoral metaphyses with bone infarcts.
Diffuse osteopenia. Thin and porous cancellous bone.
Hemolytic anemia due to enzymatic defects in heme synthesis, which results in the accumulation and increased excretion of porphyrins or porphyrin precursors. Light sensitization and severe damage to skin. Acroosteolysis, soft-tissue atrophy, skin calcifications, osteopenia, pathologic fractures.
Other rare disorders Metaphyseal dysplasia (Pyle disease), Léri-Weill dyschondrosteosis,
Melnick-Needles syndrome (including frontometaphyseal dysplasia and otopalatodigital syndromes 1 and 2), craniometaphyseal dysplasia, osteopetrosis, pycnodysostosis.
Fig. 5.68a, b Posttraumatic periosteal reaction. Subacute subperiosteal hemorrhage with periosteal cloaking (a) and, in another patient, chronic subperiosteal hemorrhage with large subperiosteal lucency and mature remodeling (b).
Table 5.42 Metaphysis: broad metaphysis with cupping and irregular cortical outline
Diagnosis
Findings
Comments
Physiologic
The ulna in infants and young children.
The distal radial metaphysis is normal with no osteopenia.
Cupping is greatest in the early healing phase. The zone of provisional ossification is obliterated. Osteopenia and coarsened trabeculae are the result of secondary hyperparathyroidism. Cortices are thinned.
Metaphyses about the knees and wrists, distal tibia and fibula, and costochondral junctions (rachitic rosary) are most severely affected.
Vitamin D–resistant rickets
Similar findings as vitamin D–deficiency rickets.
DD: chronic renal failure with secondary hyperparathyroidism, intestinal malabsorption, premature infants on long-term parenteral nutrition, Menkes syndrome with copper deficiency, infantile, hypophosphatasia, and long-term anticonvulsant therapy (barbiturates and hydantoin).
Metaphyseal bands may be solitary or multiple. MRI will show marrow replacement.
Decreased endochondral bone formation is most visible in the most rapidly growing bones. Bone pain.
Healing rickets
Irregular bands.
Irregular bands help differentiate rickets from other diseases.
Scurvy
Trümmerfeld zone. Increased signal intensity in the metaphysis on T2-weighted MRI.
Trümmerfeld zone or scurvy line is the lucent band in metaphysis more proximal to the diaphysis than the white line of Frankel at the zone of provision calcification. Metaphyseal irregularities with spurring (Pelkan sign). White lines surrounding the epiphyses. Rare in industrialized countries and widespread in areas of the world dependent on external food aid.
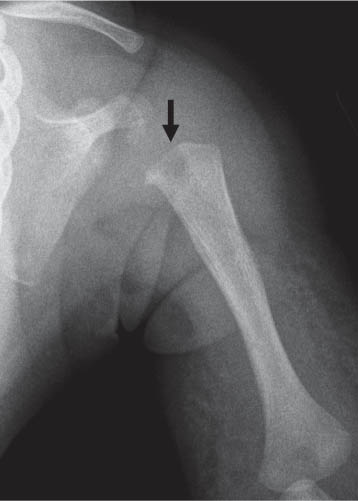
Congenital syphilis
Single or multiple metaphyseal lucent bands.
Periosteal reaction. Lucent lesion in the proximal medial tibial metaphysis (Wimberger sign). Epiphyses are usually spared.
Congenital rubella infection
Longitudinal striation of sclerotic and radiolucent areas (celery stalk appearance) at the metaphyses.
May also appear similar to other TORCH (t oxoplasmosis, o ther infections, r ubella, c ytomegalovirus, and h erpes simplex virus) infections with a more irregular pattern of sclerosis and lucency at the metaphysis.
Other TORCH infections
Nonspecific appearance seen after birth with irregular sclerosis and lucency at the metaphysis.
Hypervitaminosis D
Wide submetaphyseal lucent bands.
After long-term ingestion of high doses of vitamin D.
Fig. 5.72 Lucent metaphyseal line (arrow) in an infant with long-term care in the intensive care unit.Fig. 5.73a, b Metaphyseal lucent bands (arrows in a) in a 3-year-old boy with pre-B cell acute lymphoblastic leukemia infiltrating the bone marrow. (b) Diffuse bone marrow infiltration is seen on the T1-weighted MRI with suppression of fat in all visualized bone marrow.
Although metaphyseal corner fractures have a strong association with child abuse, imaging findings at the corners of the metaphyses may also arise from normal variation during skeletal maturation and a wide array of syndromes, dysplasias, and metabolic conditions.
Table 5.44 Metaphysis: corner fractures and spurs (see Table 5.98)
Diagnosis
Findings
Comments
Subperiosteal bone collar (normal variation)
Discrete mineralized spur at the periphery of the physis or an abrupt step-offof the metaphyseal cortex as it approaches the physis.
Osseous ring that surrounds the primary spongiosa of the metaphysis and, to a variable extent, the physis. The collar has a variety of imaging appearances that may simulate metaphyseal fractures. Most common at the knees and wrists. A follow-up radiograph may be necessary to exclude healing from trauma.
DD: neonatal rickets with hyperparathyroidism, congenital hyperparathyroidism
Obstetric injury
Extraction from a breech or armling presentation may produce traction and torsion similar to the forces occurring in child abuse.
Bone dysplasias
Follow-up radiograph will show no change in appearance, unlike the healing that would occur after trauma.
Although the underlying dysplasia is often clinically evident, several dysplasias may manifest only with modest osseous changes in early infancy (e.g., Metaphyseal chondrodysplasia, Schmid type).
Iatrogenic
Children with underlying neuromuscular disorders (myelodysplasia) may sustain metaphyseal injuries during physical therapy. Infants after orthopedic manipulation.
Osteogenesis imperfecta
In rare cases, blue sclera are absent (type IV), and osteopenia may be difficult to detect to establish a diagnosis of osteogenesis imperfecta before the incorrect diagnosis of child abuse is entertained.
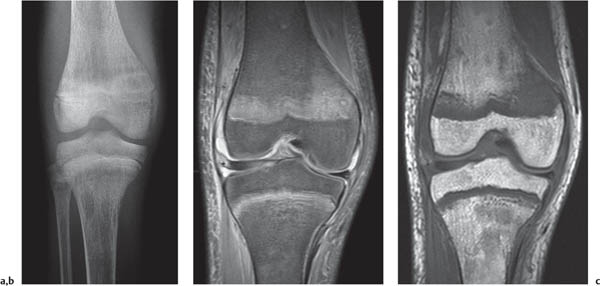
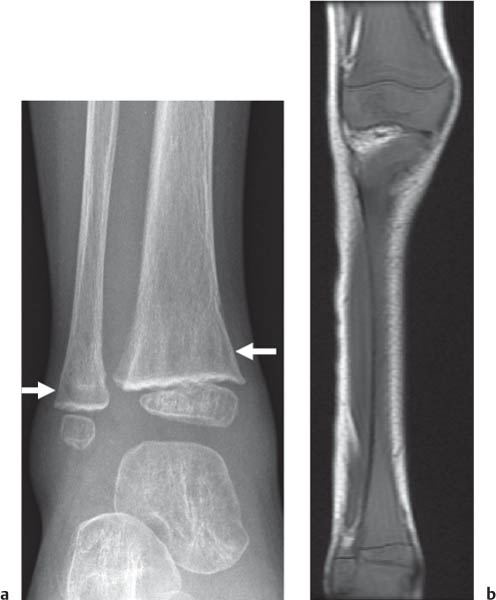
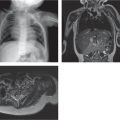
Fig. 5.74a, b Child abuse with metaphyseal corner fractures at the distal femur and proximal and distal tibia (a). (b) Whole-body STIR MRI shows the corner fractures, epiphyseal separation at the left tibia (arrow), and rib fracture (arrowhead). Note the lymph nodes in the right axilla.Fig. 5.75a, b Subacute classic metaphyseal lesion at the distal humerus (arrow in a) with healing periosteal reaction extending proximally along the diaphysis (b).Fig. 5.76a–c Metabolic metaphysis. Renal osteodystrophy with metaphyseal widening on radiography (a) and edema on T1- and T2-weighted MRI (b, c).
Symmetric distribution of very fine lines perpendicular to the physis.
Evidence of variable rates of bone growth similar to rings on a tree. Usually less dense and numerous than after a severe systemic disease (see subsequent discussion).
Healing rickets
Increased metaphyseal density.
Asymmetric ossification immediately adjacent to the zone of provisional ossification.
Horizontal sclerosis located ~1–3 cm from the physis.
Neuroblastoma
Mixed lytic and sclerotic lesion (s).
May affect metaphysis or diaphysis.
Scurvy
Normal or increased mineralization of the zone of provisional calcification on the metaphyseal side of the growth plates and surrounding the epiphyses.
Additionally, increased trabecular thickening and fine periosteal reaction.
Chronic lead poisoning
Very dense broad metaphyseal bands.
Similar changes in other types of heavy metal poisoning. Density does not represent deposition of metal but rather inhibition of osteoclasts with subsequent preferential activity of osteoblasts.
Hypoparathyroidism
Irregular zones of density in the long bones, atypical growth lines.
Metaphyseal density with generalized osteosclerosis.
Infantile hypercalcemia, supravalvular aortic stenosis, elfin face, multiple peripheral pulmonary arterial stenoses, mental retardation, and other defects.
Homocystinuria
Metaphyseal spicules.
Osteoporosis, flattening of the vertebral bodies (codfish vertebrae), scoliosis and kyphosis, bowed radius and ulna.
Fig. 5.77a, b Growth recovery lines about the ankle (a) and hind foot (arrow in b) in a 12-year-old.Fig. 5.78a–c Dense horizontal metaphyseal bands. Five months time had passed between the initial (a) and follow-up (b, c) imaging when the dense bands (arrows) developed in this child recovering from tumor therapy.Fig. 5.79 Dense metaphyseal line (arrow) from an insufficiency fracture. The insufficiency fracture has developed near old healing fractures in the fibula and tibia.Fig. 5.80 Osteopetrosis with very dense bones replacing the intramedullary space and a pathologic fracture.Fig. 5.81 Williams-Beuren syndrome. Dense femoral metaphyses (arrows) in a child with Williams syndrome.
Table 5.46 Metaphysis: perpendicular linear bands of metaphyseal lucency and sclerosis
The perpendicular view will usually reveal the exostosis.
Hypophosphatasia, infantile
Long bone bowing and characteristic Bowdler transverse spurs of the long bones.
Symmetrical central defects in the distal femoral metaphyses.
Osteopathia striata
Fine longitudinal lines in the metaphyses of long bones.
Little consequence in the long bones, but osteosclerosis in the cranial and facial bones leads to disfigurement and to disability due to pressure on cranial nerves.
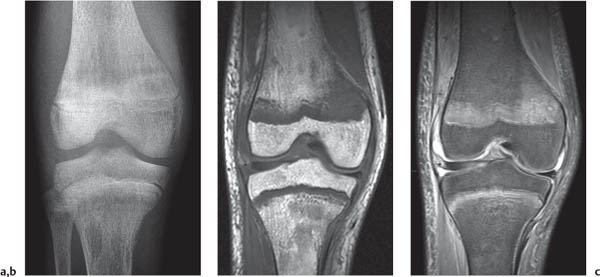
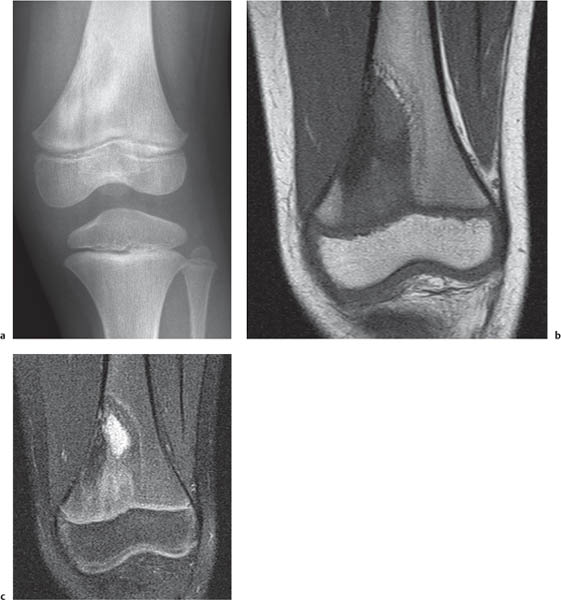
Fig. 5.82 Variation of normal. Perpendicular linear bands in the proximal femurs to be distinguished from osteopathia striata.Fig. 5.83a–c Chronic recurrent multifocal osteomyelitis. (a) AP view of the knee shows a mixed lucent and sclerotic lesion in the distal femur in a 6-year-old. (b) Coronal T1-weighted image shows replacement of fat and extension to the physis. (c) Coronal proton-density–weighted fat-suppressed image shows central increased signal intensity.Fig. 5.84 Osteomyelitis in a 1-year-old. The infection has produced a focal lucency in the proximal metaphysis of the humerus (arrow).
Only gold members can continue reading. Log In or Register to continue