Abstract
Middle mediastinal masses are usually recognized by alteration of normal mediastinal contours that may be closely related to the trachea, esophagus, great vessels, and lymph nodes. Lymphadenopathy is a common cause of a middle mediastinal mass and may be the first manifestation of lymphoma, metastases, or inflammatory diseases such as tuberculosis, fungal infections, or sarcoidosis.
Keywords
bronchogenic cyst, esophageal tumors and cyst, fungal infections, lymphoma, metastases, sarcoidosis, tuberculosis
Questions
- 1.
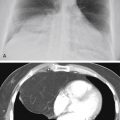
The most likely diagnosis in the asymptomatic young patient shown in Fig. 10.1 , A-C is:
- a.
Bronchogenic cyst.
- b.
Leiomyoma of the esophagus.
- c.
Carcinoma of the esophagus.
- d.
Lymphoma.
- e.
Neurenteric cyst.

Fig. 10.1
- a.
- 2.
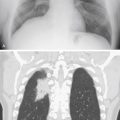
Which one of the following is the most likely diagnosis for the case illustrated in Fig. 10.2 , A-C ?
- a.
Lymphoma.
- b.
Metastases.
- c.
Primary tuberculosis.
- d.
Sarcoidosis.
- e.
Leiomyoma of the esophagus.

Fig. 10.2
- a.
- 3.
Referring to Fig. 10.3 , which of the following diagnoses may result in calcified middle mediastinal masses?
- a.
Histoplasmosis.
- b.
Tuberculosis.
- c.
Sarcoidosis.
- d.
Silicosis.
- e.
All of the above.

Fig. 10.3
- a.
- 4.
What is the most likely cause of mediastinal adenopathy in a patient with acquired immunodeficiency syndrome (AIDS) and a CD4 count of 50?
- a.
Persistent generalized adenopathy (PGL).
- b.
Tuberculosis.
- c.
Lymphoma.
- d.
Pneumocystis jiroveci pneumonia.
- e.
Kaposi sarcoma.
- a.
Discussion
The evaluation of a middle mediastinal mass requires careful consideration of the normal structures found in the middle mediastinum. 87 , 237 , 443 , 517 , 631 Based on the divisions of the mediastinum described by Felson, 150 the middle mediastinum does not correspond precisely with the classic anatomic description of the middle mediastinum. On the lateral chest radiograph, it is the area between the anterior border of the trachea and posterior border of the heart and a line drawn 1 cm posterior to the anterior border of the vertebral bodies. This area includes the trachea, bifurcation of the trachea, arch of the aorta, great vessels, pulmonary arteries, esophagus, and numerous paratracheal and peribronchial nodes. The trachea is outlined with air, and small amounts of air may be detected in the esophagus. 444 The lateral view is especially important in the evaluation of the normally lucent retrotracheal space. 171
The causes of a middle mediastinal mass can be divided into four broad categories: lymphadenopathy, primary tumors, vascular lesions, and duplication cysts ( Chart 10.1 ). When the various causes of lymphadenopathy are taken together, they are clearly the most common cause of a middle mediastinal mass.
- I.
Neoplastic adenopathy
- A.
Metastasis, including lesions derived from lung primaries 379
- B.
Lymphoma
- C.
Leukemia
- D.
Angioimmunoblastic lymphadenopathy 292
- E.
- A.
- II.
Inflammatory adenopathy
- A.
Tuberculosis 225 , 331 , 388 , 394
- B.
- C.
Blastomycosis (rare) 450
- D.
Coccidioidomycosis
- E.
Sarcoidosis
- F.
Viral pneumonia (particularly measles and cat scratch fever)
- G.
AIDS 314
- H.
Infectious mononucleosis 248
- I.
Pertussis pneumonia
- J.
Amyloidosis 246
- K.
Plague 544
- L.
Tularemia 496
- M.
- N.
Giant lymph node hyperplasia (Castleman disease) 370 , 611
- O.
Connective tissue disease (e.g., mixed, rheumatoid, lupus)
- P.
Bacterial lung abscess 482
- Q.
Mycobacterium avium complex (MAC, in patients with AIDS) 314
- R.
Anthrax 125
- A.
- III.
Inhalational disease adenopathy 175
- A.
Silicosis
- B.
Coal worker’s pneumoconiosis
- C.
Berylliosis
- A.
- IV.
Primary tumors
- A.
Lung cancer 542
- B.
Tracheal tumors
- 1.
Carcinoma
- 2.
Adenoid cystic carcinoma
- 3.
Papilloma
- 4.
Metastases
- 5.
Lipoma
- 6.
Leiomyoma 301
- 7.
Amyloid tumor
- 8.
Granular cell myoblastoma of the trachea (rare) 514
- 1.
- C.
Esophageal tumor 558
- 1.
Benign (leiomyoma) 530
- 2.
Malignant (carcinoma, leiomyosarcoma)
- 3.
Solitary fibrous tumor of the pleura 116
- 1.
- A.
- V.
Vascular lesions
- A.
Aneurysms
- B.
Aortic dissection
- C.
Distended veins (e.g., superior vena cava, azygos vein, esophageal varices) 326
- D.
Hematoma
- E.
Primary angiosarcoma (pulmonary artery)
- F.
Left superior vena cava
- G.
Aberrant right subclavian artery
- H.
Right aortic arch
- A.
- VI.
Duplication cysts
- A.
Bronchogenic or respiratory cyst (includes tracheal and some esophageal cysts) 463
- B.
Enteric cyst
- C.
Extralobar sequestration (including esophageal lung) 233
- A.
- VII.
Other
- A.
Hiatal hernia
- B.
Esophageal diverticulum
- C.
Dilated esophagus (achalasia)
- D.
Thyroid and parathyroid 121 masses that extend into the mediastinum
- E.
Cystic hygroma (lymphangioma)
- F.
Amyloidosis 430
- A.
- I.
Neoplastic adenopathy
- A.
Non-Hodgkin lymphoma
- B.
Kaposi sarcoma
- C.
Metastasis, from distant or primary lung tumors
- A.
- II.
Inflammatory adenopathy
- A.
- B.
Mycobacterium avium complex (MAC)
- C.
Fungal infections (histoplasmosis, coccidiomycosis)
- D.
Persistent generalized adenopathy (small nodes between 1 and 1.5 cm detectable on computed tomography [CT])
- A.
Middle mediastinal lymphadenopathy is most reliably identified by the detection of a mass in an area that is known to have a specific lymph node—for example, a subcarinal, right paratracheal, azygos, or ductal node ( Fig 10.4 ). Because many of the processes to be considered involve multiple nodes in the same area, there is a strong but not invariable tendency for mediastinal adenopathy to result in the appearance of a lobulated mass. The causes of middle mediastinal adenopathy greatly overlap the causes of hilar adenopathy, a condition that further contributes to the lobulated appearance of the masses.