CHAPTER 8 The most common cause of dwarfism is achondroplasia, a congenital, hereditary disease of failure of endochondral bone formation. The femurs and humeri are more profoundly affected than the other long bones, although the entire skeleton is abnormal. The spine typically has narrowing of the interpedicular distances in a caudal direction (Figure 8-1), the opposite of normal, where the interpedicular distances get progressively wider as one proceeds down the spine. I know of no other entity that has narrowing of the interpedicular distance, and I have never seen a case of achondroplasia without this narrowing. The long bones are short but have normal width, giving them a thick appearance. FIGURE 8-1 The term avascular necrosis (AVN) refers to the lack of blood supply with subsequent bone death and ensuing bony collapse in an articular surface. This condition is also called osteonecrosis. The etiology of AVN is an extensive differential that most commonly includes trauma, steroids, aspirin, sickle cell disease, collagen vascular diseases, alcoholism, and idiopathic conditions (Box 8-1).1 The radiographic appearance ranges from patchy sclerosis (Figure 8-2, A) to articular surface collapse and fragmentation (Figure 8-3). Just before collapse, a subchondral lucency is occasionally seen (Figure 8-4); however, this is a late and inconstant sign of AVN. Magnetic resonance imaging (MRI) is extremely valuable in demonstrating the presence and extent of AVN (Figure 8-2, B), even when plain films are apparently normal. MRI is currently considered the most efficacious way to evaluate a joint for AVN.2 It is useful in AVN not only of the hips but also of the knee, wrist, foot, and ankle. FIGURE 8-2 FIGURE 8-3 FIGURE 8-4 Also known as diaphyseal dysplasia, Engelmann’s disease is a congenital disorder manifested by diaphyseal cortical thickening, which primarily involves the long bones, particularly the lower extremity (Figure 8-5). Although it can be asymptomatic and incidental, children with Engelmann’s disease can have a painful, waddling gait, and the disease can progress dramatically, causing severe medullary encroachment with subsequent anemia. Hypertrophic pulmonary osteoarthropathy (HPO) is manifested by clubbing of the fingers and periostitis, usually in the upper and lower extremities (Figure 8-6), which may or may not be associated with bone pain. It is most commonly seen in patients with lung cancer, but many other etiologies have been reported, including bronchiectasis, gastrointestinal disorders, and liver disease. The actual mechanism of formation of periostitis secondary to a distant malignancy or other process is unknown. The differential diagnosis for periostitis in a long bone without an underlying bony abnormality includes HPO, venous stasis, thyroid acropachy, pachydermoperiostosis, and trauma (Box 8-2). Melorheostosis is a rare, idiopathic disorder characterized by thickened cortical new bone that accumulates near the ends of long bones, usually only on one side of the bone, and has an appearance likened to dripping candle wax (Figure 8-7). It can affect several adjacent bones and can be symptomatic. Many believe there is some relation or overlap among melorheostosis, osteopathia striata, and osteopoikilosis (mentioned later in this chapter), all of which present with varying patterns of increased cortical bone. The mucopolysaccharidoses are a group of inherited diseases characterized by abnormal storage and excretion in the urine of various mucopolysaccharides, such as keratan sulfate (Morquio’s) and heparan sulfate (Hurler’s). Affected patients have short stature, primarily from shortened spines, and characteristic plain film findings. In the spine, patients with Morquio’s syndrome have platyspondyly (generalized flattening of the vertebral bodies) with a central anterior projection or “beak” off of the vertebral body as viewed on a lateral plain film (Figure 8-8). In patients with Hurler’s or Hunter’s syndrome, platyspondyly is seen with a “beak” that is anteroinferiorly positioned (Figure 8-9) (remember “middle” beak for Morquio’s syndrome and “h
Miscellaneous conditions
Achondroplasia

 Achondroplasia. An anteroposterior (AP) plain film of the spine in this patient with achondroplasia demonstrates narrowing of the interpedicular distance (arrows) in a caudal direction, which is characteristic of this disorder. Ordinarily the interpedicular distance widens in each vertebra in a caudal direction.
Achondroplasia. An anteroposterior (AP) plain film of the spine in this patient with achondroplasia demonstrates narrowing of the interpedicular distance (arrows) in a caudal direction, which is characteristic of this disorder. Ordinarily the interpedicular distance widens in each vertebra in a caudal direction.
Avascular necrosis
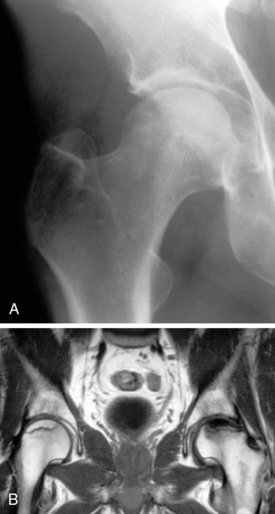
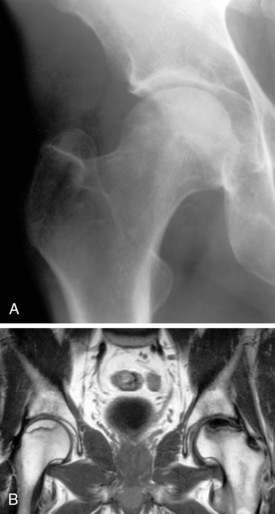
 Avascular necrosis. A, A plain film of the hip in this patient with avascular necrosis (AVN) shows faint patchy sclerosis throughout the femoral head. This is a relatively early plain film finding for AVN. B, Coronal T1-weighted image in another patient with bilateral AVN of the hips shows two different appearances with low signal on the left side and high signal on the right. Each is consistent with AVN.
Avascular necrosis. A, A plain film of the hip in this patient with avascular necrosis (AVN) shows faint patchy sclerosis throughout the femoral head. This is a relatively early plain film finding for AVN. B, Coronal T1-weighted image in another patient with bilateral AVN of the hips shows two different appearances with low signal on the left side and high signal on the right. Each is consistent with AVN.
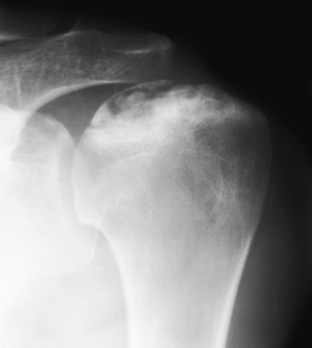
 Avascular necrosis. An AP plain film of the shoulder reveals articular surface collapse in this patient who was treated with steroids for systemic lupus erythematosus. This is an advanced stage of AVN.
Avascular necrosis. An AP plain film of the shoulder reveals articular surface collapse in this patient who was treated with steroids for systemic lupus erythematosus. This is an advanced stage of AVN.
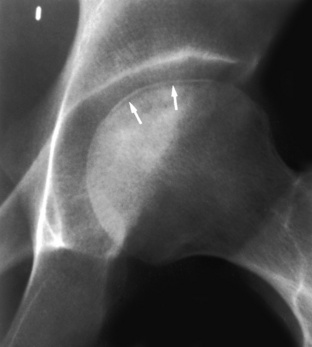
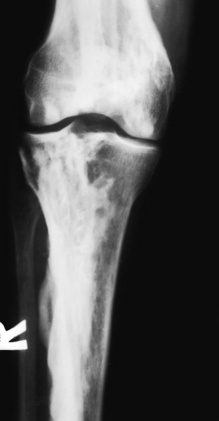
 Avascular necrosis. An AP frog-leg lateral view of the hip in this patient with sickle cell disease shows a subchondral lucency (arrows) and patchy sclerosis in the femoral head, indicative of AVN. This is a relatively advanced stage of AVN. The subchondral lucency is often better demonstrated with the frog-leg lateral view.
Avascular necrosis. An AP frog-leg lateral view of the hip in this patient with sickle cell disease shows a subchondral lucency (arrows) and patchy sclerosis in the femoral head, indicative of AVN. This is a relatively advanced stage of AVN. The subchondral lucency is often better demonstrated with the frog-leg lateral view.
Engelmann’s disease
Hypertrophic pulmonary osteoarthropathy
Melorheostosis
Mucopolysaccharidoses (morquio’s, hurler’s, and hunter’s syndromes)
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Radiology Key
Fastest Radiology Insight Engine