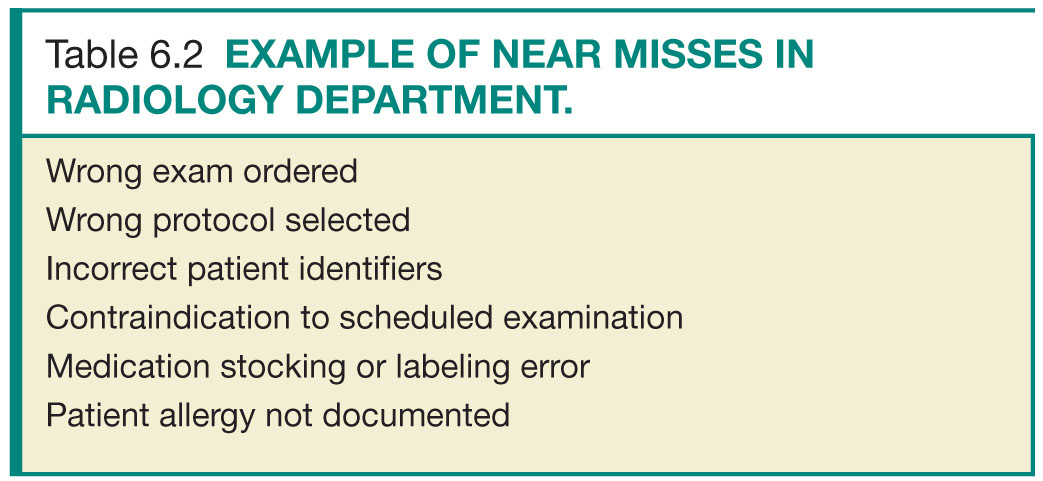
Near Misses
Near misses are safety events that do not reach a patient or result in minimal harm (Table 6.2). A more positive term is “good catch,” reflecting that the error was detected and corrected before reaching the patient. Unfortunately, near misses tend to receive less attention than sentinel events despite the fact that a number of opportunities for improvement can be garnered from studying processes and practices that result in near misses.
Medical errors can be caused by single or multiple contributing factors that include limited or lack of knowledge, insufficient experience, fatigue, carelessness, and faulty judgment.5
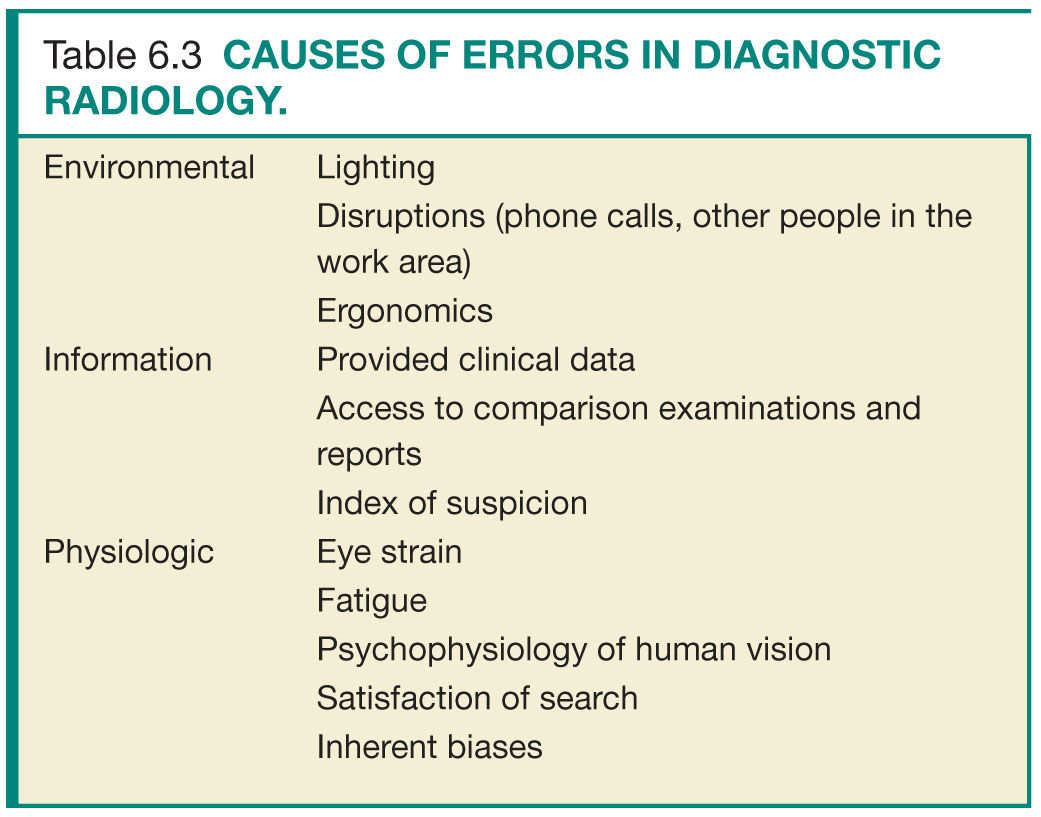
In radiology, errors can lead to delay in diagnosis and treatment, failure to recognize treatment-related complications, performing a study that is contraindicated or not indicated, or failure to adequately supervise and monitor an examination.6 Errors in diagnostic radiology are common and are often multifactorial (Table 6.3). Environmental factors such a room lighting, available clinical information, index of suspicion, comparison studies, old radiology reports,7 and psychophysiologic characteristics of human visual perception8 all play into the complex process of medical imaging interpretation.9
For image interpretation, three types of errors have been described.10 Scanning error is the failure to fixate on the area of the abnormality. Various factors can contribute to scanning error, including lack of search pattern, eye fatigue, and interruptions. Recognition error is failure to recognize the abnormality. Factors that can contribute to scanning error include eye fatigue, room ambience, lack of experience, and technical limitations (artifact, noise, etc.). Decision-making error, the most common, is the incorrect interpretation of abnormal finding as normal or a normal finding as abnormal. Another important type of observational error in diagnostic radiology is satisfaction of search, which occurs when an abnormality is overlooked because another one is found. Satisfaction of search can be associated with scanning error, recognition error, or decision-making error.
ERROR REPORTING SYSTEMS
Error reporting systems can be defined as mandatory or voluntary. Some organizations may contract with third-party vendors while other organizations develop their own error reporting systems.
Mandatory Reporting Systems
Mandatory reporting systems have the primary purpose of holding providers accountable. These focus on errors that contribute to serious injury or death. State regulatory agencies and programs typically oversee these reporting systems and have the authority to investigate specific cases and issue penalties for wrongdoing. Mandatory reporting systems serve three main functions. First, they provide a minimal level of protection to the public by ensuring that serious errors are reported, investigated, and followed up on. Second, they incentivize health-care organizations to improve patient safety under the pressure to avoid penalties and public exposure. Third, require all health-care organizations to make an investment in patient safety. Although errors reported through mandatory reporting systems represent those with greatest severity and resulting in greatest harm, these errors and complications constitute only a small fraction of errors.
Voluntary Reporting Systems
In contrast to mandatory reporting systems, which focus on accountability and corrective actions, voluntary reporting systems attempt to identify gaps in health-care delivery with the intention of fostering a culture of quality improvement. Voluntary reporting systems typically provide for event reporting into a closed system, and penalties are not assessed around a specific case.11 Near misses or events with only minimal harm are the primary focus of voluntary reporting systems. Analysis of these aggregated reports provides organizations with comparison data from their peers and can help organizations identify underlying systems problems that can contribute to patient harm. For voluntary reporting systems to be effective, attention to reported events and adequate resources dedicated to process improvement are required.
Components of an Event Report
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


