Welcome to the real world of radiology! Section A ( the real world ) contains 10 cases with the patient’s age, sex, and a brief history. Section B (the real, real world) contains 10 cases with just the patient’s age and sex. By the end of these sessions, I hope you will realize the value of a good history in interpreting images or any other consultation.
Examine the radiographs carefully.
Then summarize your radiographic findings and try to merge that with the history to come up with a logical diagnosis or differential diagnosis.
Then, click “show” to get the answer.
Audio discussions are also available where noted.
Click here to hear a discussion of Quiz 2, Part A. [INSERT AUDIO CLIP A_INTRO.MP3]
Section A (The Real World)
Case 1


History:
This is a middle-aged man with cough and fever for 3 days.
Click here to hear a discussion of the case. [INSERT AUDIO CLIP A01.MP3]
Answer:
The frontal radiograph shows alveolar consolidation at both lung bases. The heart borders are clear and the diaphragms are likewise sharp, except for the lateral chest portion of the right diaphragm. The heart and vessels are normal. The lateral chest radiograph shows the consolidation is overlapping the spine and both diaphragms are silhouetted posteriorly. There are probably also small bilateral effusions. With a history of fever and cough, this is most likely bilateral lower lobe pneumonia.
Case 2


History:
This is an older patient, after abdominal surgery.
Click here to hear a discussion of the case. [INSERT AUDIO CLIP A02.MP3]
Answers:
Image A shows a large heart and large lung volumes, suggesting underlying COPD.
In Image B , the mediastinum has shifted to the left. There is left lower lobe consolidation without an air bronchogram. There is silhouetting of the left diaphragm. The portion of the diaphragm that is seen appears elevated.
This patient has left lower lobe atelectasis, probably caused by postoperative hypoventilation and mucous plugging.
Case 3



History:
This is an older man with a cough for 2 months.
Click here to hear a discussion of the case. [INSERT AUDIO CLIP A03.MP3]
Answer:
There is an area of focal consolidation adjacent to the right heart border. The right heart border shows a silhouette sign. The lateral chest radiograph shows a triangular density overlying the cardiac shadow. This is confirmed on the CT (click to see C) scan as a triangular density in the position of the right middle lobe. Note that the major fissure on the right is displaced anteriorly.
In an older patient, collapse of a lobe, especially in the absence of symptoms of pneumonia, is most often due to endobronchial cancer. This patient had a squamous carcinoma of the right middle lobe bronchus.
Case 4


History:
This is a 44-year-old woman with recent onset of cough, fever, and sputum production.
Click here to hear a discussion of the case. [INSERT AUDIO CLIP A04.MP3]
Answer:


There is a focal area of consolidation on the lateral chest to the left heart border ( Image C *). There is a silhouette sign of the left heart border.
On the lateral chest view ( Image D *), there is a triangular-shaped density over the cardiac silhouette.
In light of the patient’s symptoms, this is most likely a community-acquired pneumonia. Note that Cases 4 and 5 are very similar in radiographic appearance. It is often the combination of the radiographic appearance, with a clinical history or physical findings, which leads to the proper diagnosis.
Case 5



History:
This is the left chest of a middle-aged man without symptoms. These findings led to a CT scan.
Click here to hear a discussion of the case. [INSERT AUDIO CLIP A05.MP3]
Answer:
On the chest x-ray, there is a soft-tissue mass that makes an obtuse angle with the chest wall. There is also some adjacent pleural thickening. Note that the adjacent rib is normal. This suggests that it is an extra pulmonary lesion, probably in the pleural space, or of the chest wall, but not involving the rib. In Image C the CT shows a low-density area bulging into the thorax with obtuse margins. The mass seems to extend between the ribs, displacing the adjacent muscles. The ribs are normal. Note that the mass is of the same density as the chest wall fat. This is a lipoma.
Case 6

History:
This is a middle-aged man with a fever. There is a chest x-ray and a cine of a CT.
Click here to hear a discussion of the case. [INSERT AUDIO CLIP A06.MP3]
Answer:
![]()
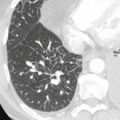
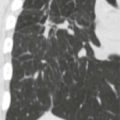
The chest x-ray shows several pulmonary nodules. There is a suggestion that they may be cavitary. (See ) The CT shows multiple cavitary pulmonary nodules. Some nodules have sharp interfaces with the lung, others are more indistinct.
In light of the patient’s fever, septic emboli or infection, such as a fungal infection, is the most likely diagnosis. Cavitary nodules also can be seen in diseases such as granulomatous polyangiitis sarcoidosis or metastatis.
Case 7


History:
This is a young man who was in an automobile accident.
Click here to hear a discussion of the case. [INSERT AUDIO CLIP A07.MP3]
Findings: