Fig. 8.1
Multiparametric prostate MRI. A 68-year-old male with biopsy-proven prostate cancer (Gleason 7 (3 + 4) and PSA 22 ng/mL). The axial T2-weighted anatomical MR image (a) shows a lesion in the right peripheral zone with extracapsular extension. This is confirmed on the ADC map showing restricted diffusion (b). The high b value (1,400) demonstrates high signal intensity within the lesion (c). The Ktrans map demonstrates an increased Ktrans compared to the contralateral site (d)
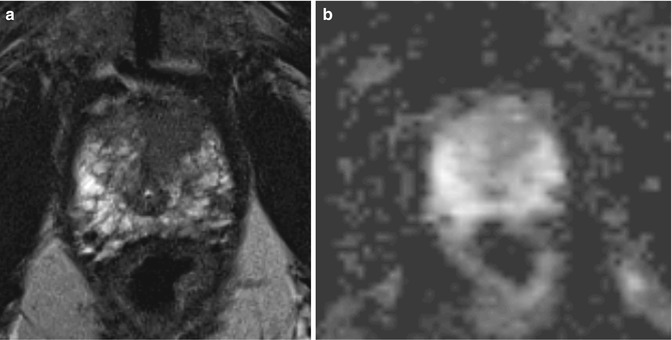
Fig. 8.2
A 70-year-old male with biopsy-proven prostate cancer in the left transition zone (Gleason 7 and PSA of 12). (a) A low-signal-intensity area in the left transition zone can be appreciated on the T2-weighted MR images. (b) The ADC map demonstrates reduced ADC in this area, however, not convincing for tumor. T2-weighted imaging is dominant in the transition zone for tumor localization
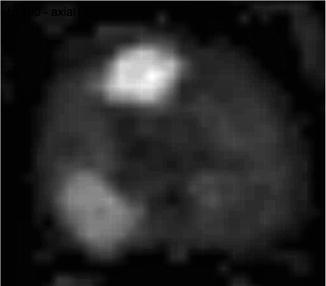
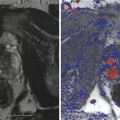
Fig. 8.3
A 62-year-old male with biopsy-proven prostate cancer in the right peripheral and transition zone (Gleason 8 and PSA of 2.1). The high-b-value MR image demonstrates high signal intensity in both right peripheral and transition zone. Histopathology revealed disease in both locations
8.3 Localization and Staging
8.3.1 Tumor Localization
MR imaging with anatomical T2-weighted MR imaging has enabled the acquisition of MR images of the prostate and its surrounding tissues with high spatial resolution. State-of-the-art 1.5 T scanners with a 16-channel phased-array coil meet the minimal requirements for clinically acceptable prostate imaging (Barentsz et al. 2012). Localization of prostate cancer with anatomical MR imaging is significantly more accurate than digital rectal examination and systematic random biopsy results in the entire prostate except for the apex (Mullerad et al. 2005). Even with an eight-channel phased-array coil, diffusion-weighted imaging outperforms anatomical imaging for tumor localization (Miao et al. 2007). The localization accuracy of dynamic contrast-enhanced MR imaging in the peripheral zone is higher compared to the transition zone. Benign prostatic hyperplasia commonly presents as fast enhancing nodules with type 3 washout curves in the transition zone (Hoeks et al. 2013). This is often mistaken for prostate cancer. Perfusion MR imaging is a very sensitive technique for the transition zone and should always be interpreted in combination with the T2-weighted images. The erased charcoal sign in the transition zone is most commonly associated with a prostate cancer. In the peripheral zone, a very fast enhancing area with a type three curve and triangular or linear signal abnormality on T2-weighted images is a typical finding for prostatitis. Diffusion-weighted imaging shows differences between prostatitis and prostate cancer in both the peripheral zone and transition zone. However, there is a significant overlap in apparent diffusion coefficients, and as a consequence the clinical applicability is questionable (Nagel et al. 2013).
8.3.2 Tumor Staging
Although a relatively high spatial resolution can be achieved within a clinically acceptable examination time, reported staging accuracy ranges from 54 to 88 % (Casciani et al. 2007; Tempany et al. 1994; May et al. 2001; Jager et al. 1996; Hricak et al. 1994). The most reliable criteria for the detection of extracapsular extension of prostate carcinoma are asymmetry of the neurovascular bundle, obliteration of the rectoprostatic angle, tumor bulge into the periprostatic fat, broad tumor contact with the surface of the capsule, an extracapsular tumor, and the radiologist’s overall impression (Schiebler et al. 1992; Outwater et al. 1994) (Fig. 8.4). Local staging of prostate cancer in the preoperative work-up of prostate cancer is cost effective and should be performed with a high-specificity reading. In attaining this specificity, however, a low sensitivity has to be considered (Jager et al. 2000). The use of dynamic contrast-enhanced MR imaging in local staging prostate cancer improves the performance of the less-experienced readers, whereas the experienced reader has no benefit (Mullerad et al. 2005). The same is true for diffusion-weighted imaging. The functional imaging technique draws the radiologist’s attention to the affected area (Bard 2009), which may improve local staging accuracy. The anatomical T2-weighted MR imaging is the most important imaging sequence for local staging. Small lesions can be appreciated on the high-resolution images, whereas diffusion-weighted imaging, proton MR spectroscopy, and dynamic contrast-enhanced MR imaging are hampered by the in-plane spatial resolution.

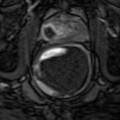
Fig. 8.4
A 56-year-old male with biopsy-proven prostate cancer (Gleason 7 (3 + 4) and PSA 16 ng/mL). (a) T2-weighted axial MR image demonstrate signal loss in the lumen of the seminal vesicle. (b) ADC map and the (c) high-b-value image confirm the findings on T2 with restriction and increased signal intensity. (d) Perfusion MR imaging demonstrates asymmetric enhancement
References
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


