Tumors of the chest wall are uncommon lesions that represent approximately 5% of all thoracic malignancies. These tumors comprise a heterogeneous group of neoplasms that may arise from osseous structures or soft tissues and may be malignant or benign. Most chest wall neoplasms are malignant and include lesions that secondarily involve the chest wall via direct invasion or metastasis from intrathoracic tumors or arise as primary tumors. More than 20% of lesions may be detected on chest radiography. This review focuses on key features of malignant and benign chest wall tumors (primary and secondary) on MR imaging examinations.
Key points
- •
Tumors of the chest wall account for only 5% of all thoracic neoplasms and represent a heterogeneous group of lesions that may arise from osseous structures or soft tissues.
- •
A majority of chest wall tumors are malignant lesions that result from direct invasion or metastasis from intrathoracic primary malignancies or arise as primary tumors.
- •
Cross-sectional imaging with MR imaging allows for lesion characterization, differentiation from non-neoplastic diseases, and delineation of disease extent.
- •
Because imaging findings may be nonspecific, a combination of clinical, radiologic, and histopathologic information is often necessary to establish the correct diagnosis.
Introduction
Chest wall tumors are uncommon lesions that represent approximately 5% of all thoracic malignancies and are less common than osseous and soft tissue tumors that occur elsewhere in the body. Thus, radiologists may be unfamiliar with the typical clinical presentation and imaging features of these rare neoplasms. Because chest wall tumors represent a heterogeneous group of lesions, several different classification schemes have been developed and may be used in clinical practice. These tumors are typically divided into categories based on the site of origin and tissue composition (osseous or soft tissue) as well as whether they are malignant or benign. Greater than 20% of chest wall tumors may be detected on chest radiography. Full characterization of these lesions is limited, however, on radiography, and cross-sectional techniques, such as multidetector CT (MDCT) and MR imaging, are the imaging modalities of choice. Although radiologic findings may be nonspecific for many of these tumors, a combination of clinical features, imaging characteristics, and histopathologic findings usually enables a definitive diagnosis, subsequently guiding further patient management. This article reviews the most common malignant and benign chest wall tumors of osseous and soft tissue origin, with emphasis placed on clinical presentation and characteristic features on MR imaging.
Introduction
Chest wall tumors are uncommon lesions that represent approximately 5% of all thoracic malignancies and are less common than osseous and soft tissue tumors that occur elsewhere in the body. Thus, radiologists may be unfamiliar with the typical clinical presentation and imaging features of these rare neoplasms. Because chest wall tumors represent a heterogeneous group of lesions, several different classification schemes have been developed and may be used in clinical practice. These tumors are typically divided into categories based on the site of origin and tissue composition (osseous or soft tissue) as well as whether they are malignant or benign. Greater than 20% of chest wall tumors may be detected on chest radiography. Full characterization of these lesions is limited, however, on radiography, and cross-sectional techniques, such as multidetector CT (MDCT) and MR imaging, are the imaging modalities of choice. Although radiologic findings may be nonspecific for many of these tumors, a combination of clinical features, imaging characteristics, and histopathologic findings usually enables a definitive diagnosis, subsequently guiding further patient management. This article reviews the most common malignant and benign chest wall tumors of osseous and soft tissue origin, with emphasis placed on clinical presentation and characteristic features on MR imaging.
Classification of chest wall tumors
Because neoplasms of the chest wall represent a heterogeneous group of lesions, no specific classification scheme is universally accepted for use in clinical practice. Most systems divide these neoplasms into several groups, however, based on site of origin, tissue composition, and whether tumors are malignant or benign. A majority of osseous tumors arise from cartilage or bone. The 2002 World Health Organization (WHO) classification system for soft tissue tumors recognizes 9 specific categories: adipocytic, vascular, fibroblastic-myofibroblastic, fibrohistiocytic, smooth muscle, pericytic, skeletal muscle, chondro-osseous, and tumors of uncertain differentiation. A classification system for soft tissue tumors suggested by Nam and colleagues includes adipocytic, vascular, fibroblastic-myofibroblastic, and fibrohistiocytic categories and adds peripheral nerve sheath and cutaneous categories; this scheme is used in this review. Additional causes of chest wall tumors, such as metastatic disease, direct invasion by lung cancer, and lymphoma, also are discussed.
Approach to chest wall tumors
When a chest wall mass is identified, a multidisciplinary approach using multiple sources of information and evaluation techniques is key to distinguishing between different tumor types, narrowing the differential diagnosis, and guiding further management. To this extent, several important features have been identified that are useful in formulating an approach: (1) patient demographics and clinical features; (2) site of chest wall involvement; (3) presence and pattern of mineralization on radiologic studies; and (4) correlation between imaging features and histopathologic findings.
Clinical presentation
Patients with chest wall tumors may be symptomatic or asymptomatic at the time of presentation. In contrast to patients with benign chest wall tumors, a majority of patients with malignant chest wall tumors are symptomatic. The most common overall clinical symptom is chest pain. In the setting of malignant tumors, the presence of chest wall pain is suggestive of osseous involvement and should raise concern for invasion. In general, malignant tumors tend to manifest as larger lesions, grow more quickly, and result in specific symptoms, such as pain, compared with benign lesions. Older patients tend to present with larger, aggressive malignant tumors, whereas younger patients tend to present with smaller benign lesions. Extrathoracic neoplasms are more likely to manifest as a growing mass than intrathoracic lesions.
Imaging evaluation
Chest radiography may be the first imaging study to suggest the presence of a chest wall mass given its widespread availability and utilization. More than 20% of lesions are visible on chest radiography. Chest radiographs are most beneficial in demonstrating the location, size, and growth rate of chest wall masses. Although mineralization, such as calcification or ossification, may be present, the high-kilovoltage technique used for radiography is not optimal for evaluation of small deposits. Such small deposits, however, may be detected on the low-kilovoltage technique used for bone radiography, which also better delineates soft tissue planes. Many benign chest wall tumors exhibit slow growth over time; therefore, these tumors may result in well-defined soft tissue planes with erosion of adjacent osseous structures.
Cross-sectional imaging techniques are more accurate in identifying and characterizing chest wall tumors. MDCT elegantly demonstrates the size and extent of local tumor as well as additional features, such as the tissue of origin, lesion morphology, and composition. Administration of intravenous (IV) contrast can be used to illustrate tumor vascularity. 2-[fluorine-18] fluoro-2-deoxy-d-glucose (FDG) positron emission tomography (PET)/CT is not routinely performed to evaluate chest wall tumors, because many primary and secondary malignancies may demonstrate increased FDG uptake. PET/CT may be used, however, to determine the presence and extent of metastatic disease and assess response to therapy.
MR imaging is the optimal modality for evaluating and characterizing neoplasms of the chest wall, because the superior soft tissue contrast and spatial resolution enable differentiation of tumor from the normal chest wall and infectious and inflammatory processes. The administration of IV gadolinium contrast is helpful in this regard. The most common sequences used to evaluate chest wall tumors include standard spin-echo and fast spin-echo sequences. In cases complicated by excessive motion, either due to proximity to the heart or from breathing, cardiac gating and respiratory compensation, respectively, can be used. Different coils can be used to optimally evaluate tumors depending on their location. For instance, surface coils are beneficial in evaluating superficial chest wall lesions, and torso coils are used to characterize tumors that have more prominent intrathoracic components.
Malignant osseous tumors
Malignant osseous tumors of the chest wall account for approximately 55% of all chest wall masses. The most common primary malignancies include sarcomas, such as chondrosarcoma, osteosarcoma, and the Ewing sarcoma family of tumors (ESFT) as well as multiple myeloma (MM) whereas metastatic disease and direct invasion from intrathoracic malignancies are the most frequent secondary causes. The overall 5-year survival of malignant osseous neoplasms is 60%.
Chondrosarcoma
Chondrosarcoma is the most common primary osseous malignancy of the chest wall and accounts for 30% of all primary malignant osseous lesions and 33% of all primary rib tumors. In addition to arising as primary tumors, these lesions have also been associated with malignant degeneration of benign chondromas, trauma, and radiation therapy. Approximately 10% of chondrosarcomas occur in the chest wall. Most tumors are identified in the anterior chest wall, in the superior 5 ribs, adjacent to costochondral junctions, or in the paravertebral regions. Origin within the soft tissues is uncommon. Although chondrosarcomas may be encountered in individuals of any age, they are typically diagnosed in the fourth to seventh decades of life and are more common in men than in women. The most common symptom reported at the time of diagnosis is a palpable and painful anterior chest wall mass.
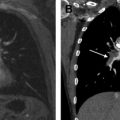
On MR imaging, the cartilage background of osteosarcomas is heterogeneous but typically iso- to hypointense to muscle on T1-weighted images and hyperintense to muscle on T2-weighted images. Regions of mineralization, such as the highly characteristic rings and arcs configuration that may be present on MDCT, are hypointense to muscle on both T1- and T2-weighted images. After the administration of IV contrast, enhancement is heterogeneous, especially at the peripheral aspect of tumors ( Fig. 1 ). Myxoid chondrosarcomas do not contain mineralization and may demonstrate markedly high signal intensity on T2-weighted images.
Osteosarcoma
Osteosarcomas are high-grade malignant mesenchymal tumors that account for 10% to 15% of malignant chest wall tumors and are most frequently diagnosed in children and adolescents. When osteosarcomas arise in a primary fashion from the chest wall, the most frequently affected structures include the ribs, clavicle, and scapula. A painful chest wall mass is usually reported at the time of presentation. Two different age peaks have been described for osteosarcomas arising from the chest wall: an osseous form that affects young adults and a less common extraosseous form that is encountered in patients older than 50 years.
On T1-weighted images, the nonmineralized regions of osteosarcomas demonstrate variable signal intensity but are often hyperintense to muscle. On T2-weighted images, the nonmineralized regions demonstrate high signal intensity. Large cystic regions may be identified within tumors. Tumor mineralization is usually hypointense on both T1- and T2-weighted imaging. Heterogeneous enhancement after the administration of IV contrast is typical ( Fig. 2 ).
Ewing Sarcoma Family of Tumors
The ESFT is a group of neoplasms that includes Ewing sarcoma and primitive neuroectodermal tumor, postulated to arise from embryonal neural crest cells and highly aggressive in nature. These tumors represent the most common primary chest wall lesions in children and young adults and the third most common overall malignant chest wall tumor. Tumors typically arise from the ribs, scapula, clavicle, and sternum and most commonly affect individuals between the ages of 20 and 30 years. All tumors included in this group contain the identical balanced reciprocal translocation between chromosomes 11 and 22, t(11; 22) (q24;q12).
On MR imaging, these tumors typically result in heterogeneous signal intensity on T1-weighted images (usually iso- or hyperintense to muscle), with regions of hemorrhage demonstrating high signal intensity. Tumors are heterogeneously hyperintense to muscle on T2-weighted images. Most lesions demonstrate intense enhancement after the administration of IV contrast ( Fig. 3 ). In general, small tumors tend to be homogeneous, whereas large lesions are more likely to demonstrate regions of heterogeneity due to hemorrhage or necrosis.
Multiple Myeloma and Plasmacytoma
Tumors comprised of malignant plasmacytes are characteristic of several malignancies, including MM, solitary plasmacytoma of bone (SPB), and extramedullary plasmacytoma (EMP). Commonly affected structures and clinical symptoms are somewhat different between these lesions. MM is most common in patients 50 to 70 years of age, whereas SPB and EMP typically affect patients 40 to 80 years of age. MM and SPB affect bones with active hematopoiesis, including the skull, thoracic skeleton, spine, pelvis, proximal humeri, and femora. Although EMP may involve any soft tissue structure, a majority are found in the upper aerodigestive tract. Typical clinical symptoms reported at the time of presentation include bone pain, renal failure, and anemia for MM; focal pain at site of tumor for SPB; and epistaxis and rhinorrhea for EMP.
MM and SPB ( Fig. 4 ) are typically iso- or hypointense to muscle on T1-weighted images and hyperintense to muscle on T2-weighted images. EMP manifests as a soft tissue mass that is low signal on T1-weighted images and high signal intensity on T2-weighted images. Diffuse enhancement of all neoplasms is typical after the administration of IV contrast.
Benign osseous tumors
Benign osseous tumors of the chest wall are less frequently encountered than malignant neoplasms. Most of these lesions are osseous or cartilaginous in etiology and include fibrous dysplasia, osteochondroma, aneurysmal bone cysts (ABCs), and giant cell tumor (GCT).
Fibrous Dysplasia
Fibrous dysplasia is a benign lesion of bone that represents the failure of mesenchymal osteoblasts to undergo normal maturation and differentiation. Lesions are monostotic in 70% to 80% of cases and polyostotic in 20% to 30% of cases. The most commonly affected osseous structures of the chest wall include the ribs, usually the lateral or posterior aspects. Involvement of the clavicle is less common. Monostotic disease is associated with an age range of 10 to 70 years, although it is most common in patients between 20 and 30 years of age. Most patients are asymptomatic; however, pathologic fractures may result in pain. Malignant transformation is rare, although development of tumors, such as osteosarcoma and fibrosarcoma, after radiation therapy has been described.
MR imaging is beneficial in demonstrating the full extent of osseous disease. Tumors usually manifest as expansile lesions that are confined to the bone. Fibrous dysplasia is iso- to hypointense to muscle on T1-weighted images and variable in signal intensity on T2-weighted images, ranging from low signal intensity to high signal intensity.
Osteochondroma
Osteochondromas are the most common benign osseous lesion and represent hamartomatous, cartilage-capped osseous protuberances that arise from affected bone. When osteochondromas occur in the chest wall, lesions are typically also encountered elsewhere within the body. The most frequently affected structures include the ribs and scapula, and osteochondromas account for 8% of all rib lesions. When occurring in the rib, there is a predilection for the costochondral junctions. Patients may present with focal rib pain or ventral scapular pain due to bursa formation. Osteochondromas may be complicated by fractures and other osseous deformities, vascular injury, neural compression, and malignant transformation. Specific features that should raise concern for malignant transformation include pain at the tumor site, osseous erosion, regions of irregular mineralization, and thickening of the cartilage cap.
Osteochondromas are isointense to the medullary cavity of the affected osseous structure on T1-weighted images. Similar to cartilaginous components of other tumors, the cartilaginous cap of osteochondroma is isointense to muscle on T1-weighted images and hyperintense to muscle on T2-weighted images. Malignant transformation should be considered if the thickness of the cartilage cap measures greater than 2 cm in adults or 3 cm in children.
Aneurysmal Bone Cyst
ABCs, which can originate as primary tumors or as secondary changes in other neoplasms, represent networks of multiple blood-filled cysts lined by fibroblasts, multinucleated giant cells, or osteoclasts. These lesions are most common in patients under 30 years of age. The most common sites of chest wall involvement include the posterior elements of the spine, such as the lamina, articular processes, and spinous processes.
Most ABCs appear as lobulated or septated masses with a well-defined low signal intensity rim on MR imaging. Heterogeneous signal intensity on both T1- and T2-weighted images is due to the presence of hemorrhagic components ( Fig. 5 ). Fluid-fluid levels may be present; however, other tumors, such as GCTs, simple bone cysts, and chondroblastomas, may also demonstrate fluid-fluid levels. ABCs may demonstrate rapid growth, osseous destruction, and extension into adjacent soft tissues; in the setting of such features, these tumors may be indistinguishable from sarcomas and other malignancies.
Giant Cell Tumor
GCTs are benign lesions composed of vascular sinuses lined or filled with abundant spindle and giant cells. These tumors are usually diagnosed between the ages of 21 and 40 years and are more common in women than in men. When GCTs occur in the chest wall, the most common location is the subchondral region of flat and tubular bones, including the sternum, clavicle, and ribs.
GCTs usually demonstrate low to intermediate signal intensity on both T1- and T2-weighted images ( Fig. 6 ). The low signal intensity may represent deposition of dense collagen and hemosiderin within the lesion. Changes similar to ABCs also may be found concurrently in GCTs. Fluid-fluid levels are less common, however, in GCTs than ABCs.
Soft tissue tumors
Malignant and benign soft tissue neoplasms of the chest wall represent a heterogeneous group of lesions that may be divided into the following groups based on the tissue of origin: adipocytic, vascular, peripheral nerve sheath, fibroblastic-myofibroblastic, fibrohistiocytic, and cutaneous.
Adipocytic: Liposarcoma
Liposarcomas are the second most common chest wall malignancy of soft tissue origin. These tumors account for approximately 15% of all sarcomas, although only 10% of involve the chest wall. Liposarcomas are most common in men between the ages of 40 and 60 years but also may affect children. Histopathologically, these tumors are composed of lipoblasts that range from poorly differentiated round cells to mature adipose tissue. Five pathologic subtypes of liposarcomas are recognized by the WHO: well-differentiated, dedifferentiated, myxoid, pleomorphic, and mixed. The most common subtype is well-differentiated liposarcoma, which represents 50% of all lesions.
Well-differentiated liposarcomas are typically composed of 50% to 75% adipose tissue, which results in high signal intensity on T1-weighted and low signal intensity on T2-weighted images ( Fig. 7 ). Depending on the volume of fat, it may be difficult to distinguish well-differentiated liposarcoma from lipoma. Several features have been identified, however, that are suggestive of well-differentiated liposarcoma; these include lesion size greater than 10 cm, thick internal septations, nodular regions of nonadipose tissue, and adipose tissue comprising less than 75% of the tumor. Nonadipose tissue components may demonstrate enhancement after the administration of IV contrast, although this is variable. One study showed that thick, irregular septations demonstrated intense enhancement, whereas thin septations showed faint enhancement. The other histologic subtypes of liposarcoma typically demonstrate less fat. For instance, pleomorphic sarcomas may contain no visible fat on MR imaging. Myxoid liposarcomas demonstrate moderately high signal intensity on T1-weighted images and high signal intensity on T2-weighted images. Dedifferentiated liposarcoma should be suspected if a previously well-differentiated liposarcoma develops areas of low signal intensity on T1-weighted images and high signal intensity on T2-weighted images and if those areas enhance after IV administration of contrast material.