, Joon Woo Lee1 and Jong Won Kwon2
(1)
Department of Radiology, Seoul National University Bundang Hospital, Seongnam, Kyonggi-do, Republic of Korea
(2)
Department of Radiology, Samsung Medical Center, Seoul, Republic of Korea
Abstract
Spinal bone marrow is composed of red and fatty marrow in varying proportions depending on age and other factors. In this chapter, we will detail the different patterns of marrow conversion in the spine and various causes of marrow inhomogeneity. We will also offer tips to aid in differentiating focal red marrow from focal metastasis. We will describe marrow proliferative, marrow replacement, and marrow depletion disorders, highlighting the MR characteristics of multiple myeloma.
Spinal bone marrow is composed of red and fatty marrow in varying proportions depending on age and other factors. In this chapter, we will detail the different patterns of marrow conversion in the spine and various causes of marrow inhomogeneity. We will also offer tips to aid in differentiating focal red marrow from focal metastasis. We will describe marrow proliferative, marrow replacement, and marrow depletion disorders, highlighting the MR characteristics of multiple myeloma.
5.1 Marrow Conversion in the Spine
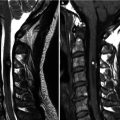
Normal marrow is composed of an intermixture of red marrow (hematopoietic marrow), yellow marrow (fatty marrow), and trabeculae in varying proportions. Fatty marrow shows high signal on T1-weighted and T2-weighted images due to its fatty composition. Red marrow shows intermediate signal intensity on T1-weighted sequences, isointense with or slightly hyperintense to the intervertebral disk, as red marrow contains both water and fat components. On T2-weighted sequences, the red marrow is intermediate in signal intensity.
At birth, there is extensive red marrow in the whole skeleton. During growth, marrow conversion from red to fatty marrow occurs in the following order: epiphyses, diaphyses, distal metaphyses, and proximal metaphyses of the long bones. In adults, red marrow remains predominantly in the axial skeleton such as the spine and in the proximal metaphyses of the long bone such as the femora. With increasing age, marrow conversion is also seen in the spine but is variable between individuals.
Four patterns of marrow conversion of red to fatty marrow in the vertebral bodies have been described on T1-weighted MR images (Ricci et al. 1990; Tall et al. 2007). In pattern 1, linear areas of high signal intensity are seen around the basivertebral vein suggestive of fatty marrow change. The remaining vertebral body is of uniform low signal intensity attributed to the red marrow. This pattern is observed in nearly half of those younger than 20 years old. In pattern 2, the conversion to fatty marrow is at the periphery of the vertebral body along the anterior and posterior corners and near the endplates, similar to that seen with Modic type 2 endplate degenerative changes. In pattern 3, diffusely distributed areas of high signal intensity are seen. Pattern 3a consists of numerous, indistinct T1 hyperintensity foci measuring a few millimeters or less. Pattern 3b consists of fairly well-marginated regions of high signal intensity ranging in size from 0.5 to 1.5 cm. Patterns 2 and 3 are seen in older individuals.
Table 5.1
Four patterns of marrow conversion in the spine
Type 1 | Linear areas of fatty marrow (T1 hyperintense) around the basivertebral vein |
Type 2 | Fatty marrow at the periphery of the vertebral body along the anterior and posterior corners and near the endplates |
Type 3a | Diffusely distributed areas of numerous, indistinct T1 hyperintense foci measuring a few millimeters or less |
Type 3b | Fairly well-marginated regions of T1 hyperintense foci ranging in size from 0.5 to 1.5 cm |
5.2 Inhomogeneous Marrow Signal on MR Images
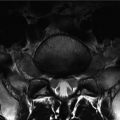
During interpretation of spinal MR images, inhomogeneous bone marrow signal within the vertebral bodies is frequently encountered. Common causes of inhomogeneous marrow signal include multiple hemangiomas, focal red marrow or focal fatty marrow deposits, as well as Modic-type endplate degenerative changes.
Hemangiomas are the most common benign tumor in the spine. The main characteristic finding of spinal hemangiomas is the presence of fatty signal (high signal intensity on T1-weighted images) within the lesion; thus most tumors of the vertebral bodies containing internal fatty signal are most likely hemangiomas. Rarely, hemangiomas can show low signal on T1-weighted images due to abundant vascular channels (aggressive or vascular hemangiomas) or internal thrombosis.
If there is a small nodule or mass within the vertebral body, the most probable diagnoses include focal red marrow deposition or metastasis. One way to differentiate focal red marrow deposition from metastasis is by evaluating the signal intensity on T1-weighted images, comparing with the intervertebral disk. Because focal red marrow contains about 40 % fat, it is isointense or slightly hyperintense on T1-weighted images to the intervertebral disk, whereas a metastatic lesion usually shows lower T1 signal intensity compared to the disk. Another point is that focal red marrow contains internal dot-like foci with preservation of trabeculation, as well as a central small fatty area. This focal region of central fat is a result of the normal centrifugal direction of marrow conversion. Focal red marrow can show mild enhancement on contrast-enhanced MR, while metastases usually enhance strongly.
Focal fatty marrow deposition can occur as part of the process of marrow conversion. The focal areas can occur anywhere in the vertebrae although these tend to be in the posterior elements, along the endplates and around the basivertebral plexus (Alyas et al. 2007).
Modic described endplate degenerative changes in MR with histopathologic correlation (Modic et al. 1988). Modic type 1 changes refer to low signal on T1-weighted and high signal on T2-weighted images, which are associated with bone marrow edema. Modic type 2 changes refer to high signal on both T1-weighted and T2-weighted images and are associated with fatty changes. Modic type 3 changes refer to low signal on both T1-weighted and T2-weighted images, associated with sclerotic changes.
Table 5.2
Focal red marrow versus focal metastasis
Focal red marrow | Focal metastasis |
|---|---|
Isointense or slightly hyperintense to the intervertebral disk on T1-weighted images | Hypointense to the intervertebral disk on T1-weighted images |
Bright central area on T1-weighted images | No central fatty area |
Patchy enhancement | Strong enhancement |
5.3 Marrow Infiltrative Disorders: Proliferative, Replacement, Depletion Disorders
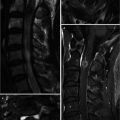
The marrow proliferative disorders result from the overgrowth of normal marrow elements, resulting in a diffusely abnormal appearance of the marrow signal on MRI. Marrow proliferative disorders include diffuse red marrow reconversion (e.g., in chronic anemia, high-altitude adaptation, following treatment for aplastic anemias), multiple myeloma, and leukemia. Multiple myeloma shows various MR features from normal, focal, variegated to diffuse involvement. Focal involvement in multiple myeloma shows similar imaging features to metastasis. The variegated involvement multiple myeloma appears as tiny nodules of variable sizes diffusely scattered throughout the entire vertebral body. These tiny nodules are of low signal on T1-weighted images and demonstrate enhancement. Disseminated bone marrow involvement of the spine shows extensive low signal intensity on T1-weighted images with diffuse enhancement. The differential diagnoses of diffuse bone marrow involvement include leukemia and lymphoma.
Marrow replacement disorders are diseases in which normal marrow elements are replaced by abnormal cells. Metastasis and lymphoma may be considered marrow replacement disorders. These are usually seen as multiple focal masses, but can be diffusely distributed. Occasionally, lymphoma can show multi-compartmental involvement of the bones, nerves, and leptomeningeal or epidural spaces. Lymphoma generally shows homogeneous signal intensity, with intermediate signal on T2-weighted images and homogeneous enhancement. If there are multi-compartmental masses with the abovementioned signal characteristics (homogenous enhancement, intermediate signal on T2-weighted images), lymphoma should be considered among the probable differential diagnoses.
Marrow depletion disorders result in the absence of normal marrow elements. MR findings show high signal on T1-weighted and T2-weighted images due to diffuse fatty marrow changes. Common causes include postradiation therapy changes, post-chemotherapy changes, and aplastic anemias (Tall et al. 2007).
Table 5.3
Marrow infiltrative disorders
Marrow proliferative disorders | Red marrow reconversion, multiple myeloma, leukemia
Related posts:Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|