Defecography by magnetic resonance (MR) imaging makes it possible to view the multiple compartments of the pelvic floor at one examination, with high-resolution images at rest and dynamic images, providing accurate evaluation of the morphology and function of the anorectal and pelvic organs and muscles, involved in pelvic floor dynamics. MR imaging of the pelvic floor identifies the diseases affecting the evacuation mechanism, providing information essential for surgical planning and choice of treatment approach. This article focuses on the MR details of the pelvic floor anatomy and the most commonly observed anatomic and functional abnormalities.
Key points
- •
Magnetic resonance (MR) imaging defecography makes it possible to evaluate the pelvic floor in its entirety with high-resolution images at rest and dynamic sequences.
- •
Defecography by MR imaging provides an accurate evaluation of the morphology and function of the anorectal and pelvic muscles and organs involved in pelvic floor dynamics.
- •
MR defecography identifies the diseases affecting the evacuation mechanism, providing information essential for surgical planning and choice of treatment approach.
Introduction
Functional disorders of the pelvic floor, such as pelvic organ prolapse, defecatory dysfunction, and urinary and fecal incontinence, represent a common health problem, especially in women. The integrity of the pelvic floor can be compromised by childbirth, pelvic surgery, obesity, constipation, age, genetic factors, and heavy physical exertion. It is estimated that pelvic floor disorder affects more than 15% of multiparous women and that 10% to 20% of patients seek medical care in gastrointestinal clinics for evacuation dysfunction. These conditions often significantly affect the quality of life and result in a variety of symptoms.
Clinical evaluation of patients with pelvic floor dysfunction is difficult. Symptoms, such as constipation, incontinence, and pain, are nonspecific and physical examination is frequently inaccurate. As a consequence, imaging is becoming popular as an adjunct tool for the assessment of pelvic floor abnormalities.
Magnetic resonance (MR) imaging is certainly an invaluable tool in the management of those patients because it provides detailed anatomic information. MR imaging makes it possible to view the pelvic floor in its entirety and multiple compartments, both at rest and dynamically.
In this article, the authors discuss the following:
- •
The MR imaging details of pelvic floor anatomy
- •
The MR imaging technique
- •
The most commonly observed anatomic and functional abnormalities
Introduction
Functional disorders of the pelvic floor, such as pelvic organ prolapse, defecatory dysfunction, and urinary and fecal incontinence, represent a common health problem, especially in women. The integrity of the pelvic floor can be compromised by childbirth, pelvic surgery, obesity, constipation, age, genetic factors, and heavy physical exertion. It is estimated that pelvic floor disorder affects more than 15% of multiparous women and that 10% to 20% of patients seek medical care in gastrointestinal clinics for evacuation dysfunction. These conditions often significantly affect the quality of life and result in a variety of symptoms.
Clinical evaluation of patients with pelvic floor dysfunction is difficult. Symptoms, such as constipation, incontinence, and pain, are nonspecific and physical examination is frequently inaccurate. As a consequence, imaging is becoming popular as an adjunct tool for the assessment of pelvic floor abnormalities.
Magnetic resonance (MR) imaging is certainly an invaluable tool in the management of those patients because it provides detailed anatomic information. MR imaging makes it possible to view the pelvic floor in its entirety and multiple compartments, both at rest and dynamically.
In this article, the authors discuss the following:
- •
The MR imaging details of pelvic floor anatomy
- •
The MR imaging technique
- •
The most commonly observed anatomic and functional abnormalities
Anatomy
A basic knowledge of the pelvic floor anatomy is fundamental to imaging interpretation and understanding of dysfunction. The pelvic floor is divided into 3 compartments: anterior, middle, and posterior. The anterior compartment contains the bladder and urethra; the middle contains the uterus, cervix and vagina; and the posterior contains the rectum and anal canal. The support of the structures arises from the attachment of the muscles, endopelvic fascia, and ligaments to the pelvic bones. In this article, the authors emphasize the female pelvic floor anatomy because functional disorders occur especially in women.
Pelvic Floor
The pelvic floor is a complex, integrated, multilayer system that provides active and passive support. The involved structures are the fascia and ligaments, the pelvic fascia, the pelvic diaphragm, and the urogenital diaphragm ( Box 1 ).
Pelvic fascia
Pelvic diaphragm
Urogenital diaphragm
Urogenital region
Fascia and ligaments provide passive support, whereas the muscles of the pelvic floor, mainly the levator ani, provide active support. The fascia is attached to the bone ring of the pelvis, with the ligament formed from fascia condensations ( Fig. 1 ).
The pelvic floor has 3 layers from superior to inferior, the pelvic fascia, pelvic diaphragm, and urogenital diaphragm, with their associated supportive structures, which are intimately to urogenital region, urethra, anal sphincter, and vaginal in women.
The components of the pelvic organ support system are integrated, and they interact and compensate each other.
Pelvic Fascia
Pelvic fascia is a delicate and special structure that envelops the pelvic viscera and maintains the support of the bladder, urethra, uterus, vagina, and rectum in their respective anatomic relationships ( Box 2 ).
Pubocervical fascia
Rectovaginal fascia
Parametrium and paracolpium
Tendineus arcus fascia
It is not a true fascia on histology and may be better described as endopelvic connective tissue. However, the structure of this fascia differs greatly from connective tissue that forms the tendon sand ligaments in other parts of the body. The endopelvic fascia comprises a meshwork of collagen, smooth muscle cells, fibroblasts, elastin, and neurovascular and fibrovascular bundles. It is a continuous sheet that goes from the pelvic viscera under the peritoneum to the pelvic diaphragm and laterally attaches to the pelvic bony ( Fig. 2 ).
The endopelvic fascia forms transverse and vertical layers of fascia. It is referred to by different names: (1) pubocervical between the bladder and the vagina; (2) rectovaginal between the vagina and rectum; (3) parametrium at the uterine level, extending from the cervix to the pelvic sidewall; (4) paracolpium at the vaginal level, extending from the vagina to the pelvic sidewall; and (5) tendineus arcus, which is a lateral condensation of the fascia.
The pubocervical fascia is a transverse anterior layer that extends from the pubis anteriorly to the cervix posteriorly, between the bladder, the urethra, and the vagina, from the pericervical ring to the perineal membrane of the urogenital triangle, which subsequently fuses to the pubic bone, and laterally inserts at the arcus tendineus fascia. The pubocervical fascia originates ligaments of the supporting system of the urethra and the bladder neck, which connect the urethra with the vagina, pubis, and levator ani. The ligaments are (1) the periurethral ligament, originating from the pubococcygeus muscle (levator ani muscle) coursing ventrally to the urethra; (2) the paraurethral ligament, connecting the lateral wall of the urethra to the periurethral ligament; and (3) the pubourethral ligament, connecting the urethra to the arcus tendineus fasciae (see Fig. 2 ). Lesions in the pubocervical fascia will result in an anterior vaginal wall prolapse, including cystocele and urethral hypermobility ( Fig. 3 ).
The rectovaginal fascia is a layer of connective tissue fused to the undersurface of the posterior vaginal wall and anteriorly to the rectum, suspended superiorly by the cervix attachment of the cardinal-uterosacral ligaments, distally attached to the perineal body, and laterally to the arcus tendineus. It is an important structure that supports the posterior compartment analogous to the pubocervical fascia in the anterior compartment. Between this fascia and the rectum lie the rectovaginal space and the pararectal fascia, which is an important plane for dissection and contains blood vessels, nerves, and lymph nodes, which supply the rectum. Lesions in the rectovaginal fascia will result in a posterior wall prolapse, including rectocele and enterocele (see Fig. 3 ).
The parametrium and paracolpium are part of the pelvic fascia at the uterus and vaginal level, respectively, extending from the cervix and the vagina to the pelvic sidewall. They are very close to the cardinal and uterosacral ligaments.
The uterosacral ligament forms the pericervical ring with fibers involving the cervix and upper vagina. The uterosacral and the cardinal ligaments together form an important, complex support system to the uterus and upper one-third of the vagina. The bilateral cardinal ligaments blend laterally with the parietal fascia of the pelvic sidewall muscles and the uterosacral ligaments with the presacral fascia ( Fig. 4 ). Lesions in the pericervical rings promote uterus and vaginal prolapse.
The arcus tendineus fascia has 2 dense aggregations of the fascia, the arcus tendineus fascia pelvis and the arcus tendineus levator ani, which provide important passive lateral support. The arcus tendineus fascia pelvis provides lateral anchoring for the anterior vaginal wall where it supports the urethra, whereas the arcus tendineus levator ani provides anchoring for the levator ani muscles.
Although the arcus tendineus fascia is too small to be visualized, its position can be inferred from the angle formed between the levator ani and the surface of the internal obturator muscles.
Pelvic Diaphragm
The pelvic diaphragm comprises the levator ani and coccygeus muscles ( Box 3 ).
| Levator ani muscle | |
| Pubococcygeus muscle | Pubovaginal, puborectal, and pubococcygeal muscles |
| Iliococcygeus muscle | |
| Coccygeus muscle |
The levator ani is the major muscle of the pelvic diaphragm, which maintains a constant basal tone and closes the urogenital hiatus, preventing incontinence and prolapse (see Fig. 1 ).
It is attached to the pubis and laterally to the arcus tendineus levator ani. This muscle is formed by inseparable parts of a single unit. However, several segments of the levator ani have been described in terms of their visceral insertions, such as the paired iliococcygeus and pubococcygeus muscles.
The ventromedial part of the levator ani, called the pubovisceralis or pubococcygeus muscle, is a thick, slinglike bundle of fibers arising from the inner aspect of the pubis, passing beside the urethra, vagina, and anorectum, and attaching to the vagina and anorectum ( Fig. 5 ).
The slinglike configuration of the ventromedial part of the pubococcygeal muscle makes this muscle an important component of the pelvic floor involved in the genesis of prolapse and urinary incontinence. Tonic contraction of the two parts of this muscle closes the urogenital and anorectal hiatus, which provides a supportive platform during normal activity and standing as well as a contraction reflex to increased intra-abdominal pressures.
The pubovaginal, puborectal, and pubococcygeal muscles compose this muscle. The pubovaginal muscle has a horseshoe shape, inserts in the lateral and posterior vagina wall, and helps to support the vagina. The puborectal muscle suspends the rectum at the anorectal junction, with a slinglike configuration around the anal canal and rectum. It controls the descent of the feces and is considered part of the external anal sphincter. The pubococcygeal part is the larger portion; is Y shaped, inserting on the coccyx (the levator plate); and also helps control the passage of stool (see Fig. 5 ; Fig. 6 ). Between their lateral components there is a space (the levator hiatus) that contains the urethra, vagina, and rectum.
The iliococcygeus muscle is the less dynamic levator ani muscle. It is located above the pubococcygeal muscle, originates from the arcus tendineus levator ani along the lateral pelvic sidewalls and extends posterior to the rectum, working as a musculofascial layer (see Figs. 5 and 6 ).
The coccygeus muscle is a less active muscle that is posterior to the levator ani and extends from the ischial spines to the lateral margins of the coccyx. These muscles are readily visible on MR imaging (see Fig. 6 ).
The sacral nerve roots, S2 through S4, innervate the levator ani via the pudendal nerve. These roots cross the pelvic floor and are stretched and compressed during labor, increasing the chance for injury.
Urogenital Diaphragm
The urogenital diaphragm, also called the deep perineal space or perineal membrane , has a horizontal configuration, situated caudal to the pelvic diaphragm, superior to the superficial perineal pouch, and anterior to the perineal body and external anal sphincter. It has a triangular configuration from the anterior and lateral pubic bone attachments (pubic simphysis and ischiopubic rami) to the posterior perineal body.
It is comprised of several muscles. The primary muscle of the urogenital diaphragm is the deep transverse muscle of the perineum, which originates at the inner surface of the ischial ramus, extends across the perineal membrane, and is readily visible at MR imaging. The other muscles compose the urethral and urethrovaginal sphincter ( Fig. 7 ).
The urogenital diaphragm has attachments to surrounding structures, including the vagina, perineal body, external anal sphincter, and bulbocavernous muscle.
Urethra
The female urethra is approximately 4.5 cm long and exhibits a ventral concavity behind the pubic bone. Two-thirds of the urethra is above the levator ani (pelvic diaphragm). In continent patients, the normal position of the urethra should be entirely retropubic, above or at the inferior pubic level.
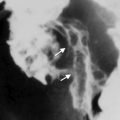
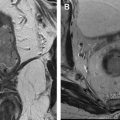
In patients presenting with stress incontinence, a short urethra as well as an inferior translation of the urethra, with the lower segment of the urethra lying below the pubis, may be demonstrated (see Fig. 3 ; Fig. 8 ).
The mucosa and submucosa and the internal and external sphincter compose the urethra and can be readily visible at high-resolution MR imaging in almost all individuals (see Fig. 8 ).
The proximal one-third of the urethra is lined with pseudostratified columnar epithelium. The folds of urothelial tissue, with rich submucosal vascular plexuses, mucosal secretions, and urethral smooth muscle, all contribute to passive urethral closure.
The urethral sphincter is comprised of involuntary inner smooth muscle that is continuous with the bladder as well as the voluntary external sphincter (rhabdosphincter), which is comprised of striated muscle. The inner smooth muscle sphincter extends throughout the proximal two-thirds of the urethra, and its tension is distributed relatively uniformly and contributes to about one-third of the intraurethral pressure. The smooth muscle of the urethra has high signal intensity on T2-weighed MR images and demonstrates enhancement after intravenous administration of contrast medium. This finding is probably caused by the specific histologic characteristics of smooth muscles (see Fig. 8 ). Lesions in the proximal sphincter muscle promote widening of the proximal urethra at the vesicle neck, called funneling ( Fig. 9 ).
Urethral and Bladder Neck Supporting Structures
Fascia and ligament support of the urethra and the bladder neck is vital to preserve urinary continence ( Box 4 ).
Periurethral ligament
Paraurethral ligament
Pubourethral ligament
Related posts:
 Posttreatment Evaluation of Central Nervous System Gliomas
Clinical Applications of Functional MR Imaging
Breast Magnetic Resonance Imaging
Posttreatment Evaluation of Central Nervous System Gliomas
Clinical Applications of Functional MR Imaging
Breast Magnetic Resonance Imaging
 MR Enterography for the Assessment of Small Bowel Diseases
MR Enterography for the Assessment of Small Bowel Diseases
 Magnetic Resonance Imaging of Rectal Cancer
Multiparametric Magnetic Resonance Imaging of the Prostate
Magnetic Resonance Imaging of Rectal Cancer
Multiparametric Magnetic Resonance Imaging of the Prostate
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


