The quality of the medical imaging is a key component for accurate disease diagnosis. Optimizing image quality while maintaining scan time efficiency and patient comfort is important for routine clinical MRIs. In this article, we review both practical and advanced techniques for achieving high image quality, especially focusing on optimizing the trade-offs between the image quality (such as signal-to-noise and spatial resolution) and acquisition time. We provide practical examples for optimizing the image quality and scan time.
Key points
- •
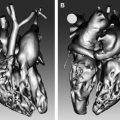
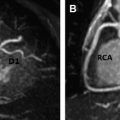
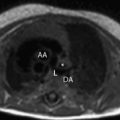
Cardiac MRI provides images with a variety of tissue contrasts, which can be exploited in the diagnosis of different cardiac conditions.
- •
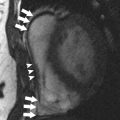
A major limitation in cardiac MRI is motion caused by the beating heart and respiration, which further constrains the trade-offs between the image quality and acquisition time.
- •
Utilization of multiple-channel coils generally provides improved image quality, and higher field strength scanners provide higher signal-to-noise ratio.
Introduction
Cardiac MRI provides images with a variety of tissue contrasts and this can be exploited in the diagnosis of different cardiac conditions. All of these contrasts require sufficient image quality to provide accurate diagnoses. Image quality in MR is based on the underlying MR physics, and usually requires trade-offs between the signal-to-noise ratio (SNR), spatial resolution, acquisition time, and so on. A major limitation in cardiac MRI is the motion caused by the beating heart and by respiration, which further constrains the trade-offs. The utilization of multiple-channel coils generally provides improved image quality, and higher field strength scanners provide higher SNR. In this paper, we introduce current practical approaches to optimize cardiac MRI quality and scan time. We review motion compensation methods, acceleration techniques, and practical examples for optimizing the image quality and scan time.
Introduction
Cardiac MRI provides images with a variety of tissue contrasts and this can be exploited in the diagnosis of different cardiac conditions. All of these contrasts require sufficient image quality to provide accurate diagnoses. Image quality in MR is based on the underlying MR physics, and usually requires trade-offs between the signal-to-noise ratio (SNR), spatial resolution, acquisition time, and so on. A major limitation in cardiac MRI is the motion caused by the beating heart and by respiration, which further constrains the trade-offs. The utilization of multiple-channel coils generally provides improved image quality, and higher field strength scanners provide higher SNR. In this paper, we introduce current practical approaches to optimize cardiac MRI quality and scan time. We review motion compensation methods, acceleration techniques, and practical examples for optimizing the image quality and scan time.
Cardiac and respiratory motion
Central to cardiac MRI is how to address the cardiac and respiratory motion. These two sources of motion are commonly managed independently to reduce image artifacts.
Cardiac Triggering
Cardiac MR images are typically reconstructed from data acquired over several heart beats. To account for cardiac motion the acquisition is synchronized with the echocardiographic signal. Morphologic, single time frame images are commonly acquired by acquiring multiple data samples during mid diastole when the heart has minimal motion. This allows for a relatively long temporal window with minimal motion artifacts, resulting in a shorter acquisition time. For functional time resolved data, the trade-off between temporal window and the total acquisition time becomes more apparent. A higher temporal resolution requires a narrower temporal window for each time frame, which requires a longer total acquisition time. On the other hand, lowering the temporal resolution widens the temporal window used to reconstruct the images, which makes it more prone to temporal blurring.
Prospective and Retrospective Modes
Time resolved cardiac image can be acquired in two different modes: Prospective or retrospective. In prospective imaging, data acquisition starts at the detection of the echocardiographic trigger and data are acquired for a predefined number of temporal phases, after which the acquisition is idle until the next trigger occurs. The predefined number of temporal phases is prescribed to cover an interval that is slightly shorter than the duration of the cardiac cycle to ensure that the system is ready for the next trigger. If the number of phases is low, the acquisition is limited to the early parts of the cardiac cycle, and if the number is too high, the acquisition may continue into the next cardiac cycle, thereby missing the trigger of that cardiac cycle. Missed triggers result in longer acquisition times. Retrospective acquisition, on the other hand, does not require a predefined number of time frames as the data are sorted after they are acquired. Furthermore, retrospective sequences run continuously, without any breaks in data acquisition between cardiac cycles, and the steady state can therefore be preserved.
Respiratory Motion
The heart is located next to the diaphragm, and respiration is therefore a major cause of motion artifacts in cardiac MRI. Analogous to cardiac motion, the remedy for respiratory motion is to acquire data at certain stages in the respiratory cycle. This can be achieved by breath-holds, navigator gating, or pneumatic bellows triggering.
Breath-hold methods are a simple and reliable means to minimize respiratory motion as long as the acquisition time is sufficiently short. However, patients often find even short breath-holds challenging. Furthermore, to cover an image volume, multiple breath-holds are usually required, which may result in slice misregistration error owing to the difficulty in consistently reproducing the same breath-hold position. To obtain short breath-holds, the breath-hold duration can be reduced using acceleration techniques described herein.
Navigator gating is a suitable option for sequences that require longer acquisition time. In navigated sequences, a separate readout is introduced to detect the movement of the diaphragm. A threshold is set for the maximum allowable excursion of the diaphragm through the acquisition, and data acquired outside that threshold are rejected and reacquired when the diaphragm returns back within the threshold. A narrow acceptance window therefore reduces the extent to which respiration degrades image quality, but increases total acquisition time. Navigator gating is a relatively accurate method for tracking respiratory motion, because it measures the actual displacement of the diaphragm. However, it continuously interrupts data acquisition, which breaks the steady state of the readout and may result in artifacts.
Acceleration
Compared with other medical imaging modalities such as ultrasonography and computed tomography, MR imaging is relatively time consuming, resulting in patient discomfort, motion-related artifacts, or limitations of imaging capabilities. The speed of the acquisition is fundamentally limited by physical and physiologic constrains. The most common approach used to accelerate the acquisition is therefore to reduce the amount of data acquired to reconstruct an image. However, the missing information that results from data undersampling causes artifacts in the reconstructed image. The goal of different acceleration methods is therefore to recover images with minimal artifacts, even in the presence of undersampled data.
Partial Acquisition and Non-Cartesian Acquisition
Most of the image energy is concentrated around the low frequency k-space center, whereas the high-frequency outer k-space contains less visual information. This can be exploited to reduce the acquisition time. One commonly used method is partial Fourier acquisition, which takes advantage of the symmetry properties of k-space. In this method, only one half of k-space is fully sampled in the phase or the slice encoding direction. With this method, nearly 50% of k-space need not be explicitly acquired but can be mathematically reconstructed, correspondingly reducing the total acquisition time. Instead of sampling the data uniformly, non-Cartesian acquisitions such as spiral and radial sampling can be designed to accelerate scan time by undersampling the outer portions of k-space and sufficiently or overly sampling the central k-space.
Sliding Window, Keyhole, Time-Resolved Imaging of Contrast Kinetics
For dynamic imaging with multiple time frames, the data can be undersampled by exploiting redundancies in the temporal domain, generally called as k–t methods. View sharing is a commonly used method to accelerate time-resolved acquisitions. The k-space is interleaved into multiple segments, and the time frames are reconstructed by sharing data with adjacent time frames. Usually, the k-space center is acquired at each time frame and the high frequencies are interleaved. The fully sampled high-frequency data are combined from all the time frames and shared for all the frames.
Parallel Imaging
Each coil element in a multiple receiver coil has its unique spatial location, and when combined that data contain spatial redundancies. In parallel imaging these spatial redundancies are exploited to reconstruct images from undersampled data. In theory, the greatest acceleration factor that can be achieved is of the order of the number of the coil elements. In practice, the SNR loss related to the parallel acquisition often limits the achievable acceleration factor. Clinically used parallel imaging methods include sensitivity encoding for fast MRI (SENSE) and generalized autocalibrating partially parallel acquisitions (GRAPPA), which have various names depending on the vendors. Parallel imaging also allows combination with k–t methods.
Compressed Sensing
Recently, the compressed sensing technique has been introduced into the field of MRI to achieve scan time acceleration by recovering images with undersampled data. Compression techniques are commonly used in applications such as MP3 audios and JPG images. Similarly, under certain constraints, the MR images can be compressed with specific transformations and can be represented by a small portion of the data. This permits the user to acquire less data (shorter scan time) but maintain sufficient image quality. Furthermore, the compressed sensing technique can also be combined with parallel imaging and k–t techniques, achieving high acceleration factors.
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


