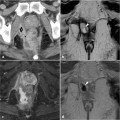
Fig. 2.1
a Axial T1-weighted image. b Axial T2-weighted image shows the complex of internal and external anal sphincters: IAS (circle), ISS (thin arrow), and EAS (thick arrow)

Fig. 2.2
Coronal T1-weighted image. The three different portions of the EAS: deep (thick arrow), subcutaneous (circle), and superficial (thin arrow)
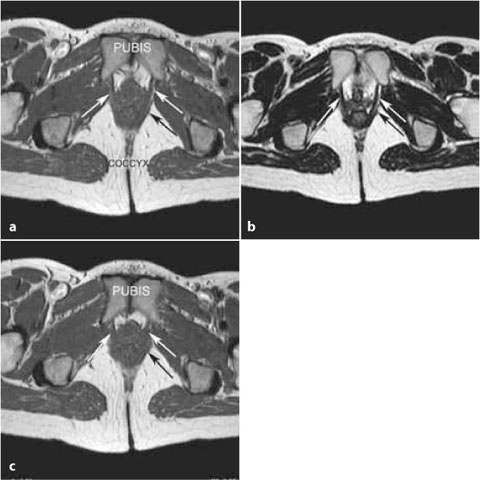
Fig 2.3
a Axial T1-weighted image. b Axial T2-weighted image on the same plane. c Caudal plane, T1-weighted image: puborectalis muscle (white arrows), pubococcygeal muscle (black arrow)
External anal sphincter (EAS). The striated muscle of the EAS continues superiorly to form the levator ani and the puborectalis. The EAS can be divided craniocaudally in three parts: deep, superficial, and subcutaneous (Fig. 2.2; see also Fig. 2.11). The middle third of the EAS surrounds the inferior portion of the IAS and is connected anteriorly to the tendinous center of the perineum and posteriorly to the anococcygeal ligament. While the EAS maintains only 15% of resting anal tone, its strong voluntary contraction is fundamental for defecation. Surgical division of the EAS can lead to incontinence.

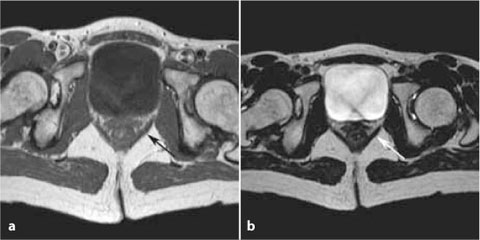
Fig. 2.4
Axial T2-weighted image. Pubococcygeal muscle (black arrow), iliococcygeal muscle (white arrow)
Fig. 2.5
a Axial T1-weighted image. b Axial T2-weighted image: iliococcygeal muscle (arrow)
Levator ani. The three muscles that form the levator ani are, from medial to lateral: the puborectalis (Fig. 2.3 a-c), the pubococcygeal (Figs. 2.3, 2.4 and 2.6), and the iliococcygeal (Figs. 2.4– 2.6). They support the viscera of the pelvic cavity, coordinate defecation-related functions, and join the coccygeal muscle to
form the pelvic diaphragm. The puborectalis muscle begins at the back of the pubis and from the top end of the urogenital diaphragm, continuing posteriorly on the contralateral side to form a U-shaped puborectal sling, located at the anorectal junction. Subsequently, it is connected with the deep layer of the EAS. The puboperinealis is the anterolateral continuation of the puborectalis; it has a rounded triangular shape and is closely related to the bladder floor and the membranous urethra.
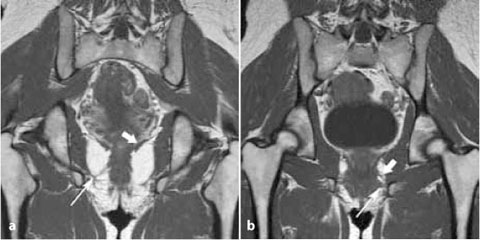
Fig. 2.6
Coronal T1-weighted image. a Dorsal plane: iliococcygeal muscle (thick arrow), pubococcygeal muscle (thin arrow). b Ventral plane: puborectalis muscle (thick arrow), superficial transverse perineal muscle (thin arrow)
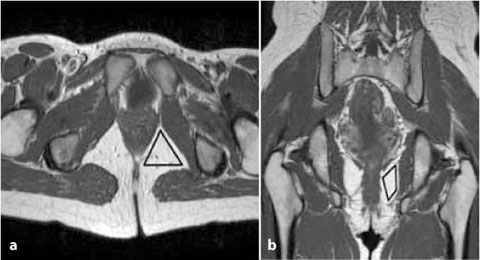
Fig. 2.7
Ischioanal space shown on an axis T1-weighted image (triangle in a) and coronal T1-weighted image (diamond in b)
Ischioanal space (IA). Triangular in shape, it lies laterally to the EAS and caudally to the levator ani muscle (Fig. 2.7a, b).
Perineal body. This structure is larger in women than in men because it protects the EAS during childbirth. Also in women, it separates anatomical structures located between the posterior distal wall of the vagina and the anterior anal canal. In men, the perineal body is not well visible because it is strictly connected to the EAS and to the perineal muscles (Fig. 2.8).
Superficial transverse perineal muscles. On the axial plane, this muscle is well-visualized as a wide and thin muscular layer cranial to the anterior EAS and connected to the perineal body. In the coronal plane, the left and right superficial transverse perineal muscles are separated medially by the bul- bospongiosus muscle and insert laterally into the fascia of the ischiocavernous muscle. These muscles serve as the bony anchor for all perineal structures (Figs. 2.6, 2.8; also see Fig. 2.12).
Anococcygeal ligament. A ventral layer extends from the sacral fascia to the common longitudinal layer of the anal canal, while a dorsal layer extends between the coccyx and the EAS (Figs. 2.9, 2.10).
Superficial postanal space




Related posts:




Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
