Anatomy, embryology, pathophysiology
- ◼
After the sixth week of gestation, in the absence of a Y chromosome, the paired Müllerian (paramesonephric) ducts begin to form in female neonates.
- ◼
Over the ensuing weeks, the two Müllerian ducts fuse with a resultant cervicouterine septum formed in between them. This septum is subsequently resorbed, creating a fully patent uterine cavity.
- ◼
Complete fusion of the Müllerian ducts results in formation of the uterus with a single cavity, fallopian tubes, cervix, and upper two-thirds of the vagina. The ovaries and lower third of the vagina are not formed by the Müllerian ducts.
- ◼
Failure of: (1) formation, (2) fusion, and/or (3) septal resorption results in Müllerian duct anomalies (MDAs).
- ◼
Including the most benign variant (arcuate uterus), the estimated prevalence of MDAs is 5.5% in the general population and up to 24.5% in patients with miscarriage and infertility.
- ◼
Renal anomalies are associated with MDAs in approximately 30% of cases.
Techniques
Ultrasonography
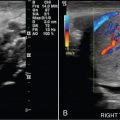
Ultrasonography (US) is a readily-available, fast, cost-effective, and radiation neutral initial screening modality for suspected female pelvic disorders. The recent advent of higher resolution techniques and advanced imaging, such as three-dimensional ultrasound (3D US) ( Fig. 35.1 ), has made evaluation of MDAs via US more accurate, rivaling the accuracy of magnetic resonance imaging (MRI).

Hysterosalpingography
Hysterosalpingography (HSG) provides a unique, dynamic evaluation of the uterine cavity and fallopian tubes via real-time contrast opacification of these structures. It confirms patency of the fallopian tubes, as well as the shape of the uterine cavity, which can secondarily infer MDAs. HSG, however, by itself is incomplete in the evaluation of uterine contour, uterine septal abnormalities, and structures that do not communicate with the cannulated cervix.
Magnetic resonance imaging
MRI offers superior anatomic imaging of the female pelvic organs because of its high image contrast, allowing for delineation of the uterus (including the myometrium, junctional zone, and endometrium), cervix, vagina, and ovaries with relative ease.
T2-weighted imaging
- ◼
The workhorse of female pelvic MRI, because of its image contrast and resultant ability to separately delineate the endometrium, myometrium, and the intervening junctional zone, as well as ovarian follicles and stroma for superb adnexal evaluation.
- ◼
Obtained in three planes for cross-correlation, augmenting certainty with respect to imaging findings identified in a single plane.
- ◼
Additional oblique planes can be prescribed during scan time to enable better visualization of the uterine cavity and contour of the uterine fundus ( Figs. 35.2 and 35.3 ).

Fig. 35.2
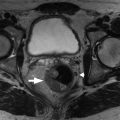
Oblique coronal imaging of the uterus. The full extent of a fibrous septum ( arrow ) of a septate uterus (and other congenital anomalies) is well delineated by orienting the imaging plane along the long axis of the uterus to obtain an oblique coronal image.
(From Roth C, Deshmukh S. Fundamentals of Body MRI , ed 2. Philadelphia: Elsevier; 2016.)

Fig. 35.3
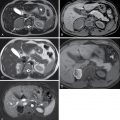
T-shaped uterus. A, Obliquely coronally reformatted T2-weighted image in a 47-year-old woman with a history of fetal diethylstilbestrol exposure elegantly portrays the aberrant anatomy that is less clearly rendered with coronal (B), sagittal (C), and axial (D) planes prescribed orthogonally to the axes of the body.
(From Roth C, Deshmukh S. Fundamentals of Body MRI , ed 2. Philadelphia: Elsevier; 2016.)
Diffusion weighted imaging
- ◼
Allows for additional certainty with respect to ovary detection, as they typically restrict diffusion.
- ◼
Provides additional diagnostic information regarding incidental lesions in the pelvis.
T1-weighted fat-suppressed dynamic contrast enhanced imaging
- ◼
DCE allows for additional certainty with respect to ovary detection, as ovarian follicles demonstrate thin peripheral enhancement.
- ◼
The endometrial lining of the uterus and any septum, if present, will demonstrate enhancement.
- ◼
Provides additional diagnostic information regarding incidental lesions in the pelvis.
Protocols
Protocol considerations
Protocols for optimal evaluation of suspected MDAs need clear anatomic delineation of the endometrial canal, fallopian tubes, and uterine fundus, which are the key structures differentiating the various MDAs.
Suggested ultrasonography protocol
- ◼
Timing: if MDAs are suspected, perform the US late in the cycle when the endometrium is thickest for optimal evaluation (routine US is performed after menstruation when the endometrium is thin).
- ◼
Images:
- ◼
Transvaginal axial and sagittal still and cine images through the entire uterus.
- ◼
3D US, if available, to give a complete picture of the uterine and endometrial shape and fundal contour.
- ◼
Suggested hysterosalpingography protocol
- ◼
Preprocedure: screen for contraindications (infection, contrast allergy, last menstrual period greater than 12 days prior making pregnancy status indeterminate) and obtain informed consent.
- ◼
Procedure:
- ◼
Patient placed in lithotomy position.
- ◼
Bimanual examination performed to locate the cervix or cervices.
- ◼
Speculum is inserted and cervix localized. Perform additional maneuvers in patients with suspected MDAs or abnormal bimanual examination to examine the vagina for an additional cervix.
- ◼
The cervix or cervices are separately cleaned and cannulated using a small catheter. Occasionally, a metal or plastic dilator is needed to advance the catheter.
- ◼
Catheter balloon is inflated with saline in the cervix or lower uterine segment to occlude contrast outflow.
- ◼
Speculum is removed.
- ◼
- ◼
Images:
- ◼
Anteroposterior preinjection.
- ◼
Anteroposterior early filling of uterus during slow injection.
- ◼
Anteroposterior late filling of uterus and fallopian tubes.
- ◼
Left and right posterior oblique after spilling of contrast through fallopian tubes.
- ◼
Anteroposterior “pull-down” coronal view, while pulling on the catheter under tension, to examine the endometrial canal in its entirety.
- ◼
Anteroposterior lower uterine segment view, while deflating the balloon and injecting, to reveal pathology previously obscured by the catheter balloon.
- ◼
Suggested magnetic resonance imaging protocol
- ◼
Abdomen
- ◼
Axial T1-weighted without fat suppression: for associated renal anomalies.
- ◼
- ◼
Pelvis
- ◼
Axial T2-weighted without fat suppression.
- ◼
Coronal T2-weighted without fat suppression.
- ◼
Sagittal T2-weighted without fat suppression.
- ◼
Oblique coronal T2-weighted without fat saturation (imaging plane prescribed by a radiologist or experienced technologist) on sagittal T2-weighted images, parallel to the long axis of uterus through the uterine fundus.
- ◼
T1-weighted in and out of phase.
- ◼
Diffusion weighted imaging (b = 100, 500, 1000) with apparent diffusion coefficient (ADC) map.
- ◼
T1-weighted with fat suppression, precontrast.
- ◼
Axial.
- ◼
Coronal.
- ◼
Sagittal.
- ◼
- ◼
T1-weighted with fat suppression, postcontrast.
- ◼
Sagittal dynamics (×4).
- ◼
Axial high resolution.
- ◼
Coronal high resolution.
- ◼
- ◼
Specific disease processes
Agenesis and hypoplasia
A result of failure of early formation of both Müllerian ducts, agenesis and hypoplasia will present with primary amenorrhea or cyclic pelvic pain related to hematocolpos or hematometra. This has also been termed Mayer-Rokitansky-Küster-Hauser syndrome.
Hysterosalpingography
- ◼
Rarely done as there will be an abnormal or absent cervix on clinical examination.
- ◼
If performed, agenesis will be readily evident upon attempted cannulation as nonvisualization of a cervical os. Hypoplasia will be evident during examination to the extent the cervical development has been affected.
Ultrasonography
- ◼
In general, there is poor visualization of the uterus, which will prompt additional imaging with MRI.
Magnetic resonance imaging
- ◼
Demonstrates a complete or partial lack of the upper vagina, cervix and uterus ( Fig. 35.4 ).