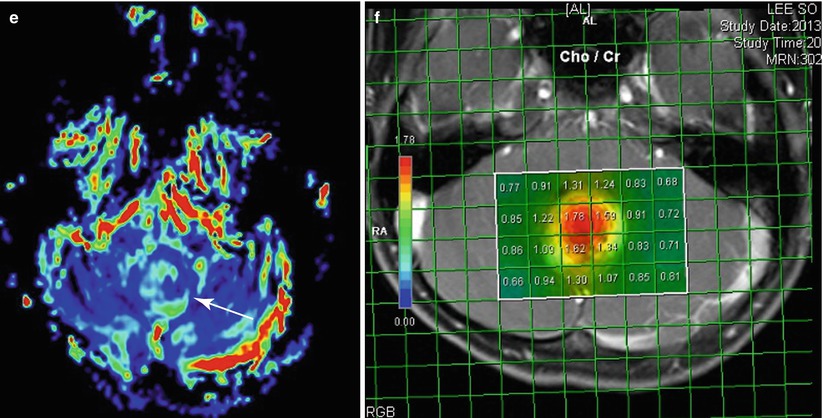
Fig. 4.1
Cerebellar pilocytic astrocytoma in a 7-year-old girl. (a) CT scan shows hypoattenuated mass (arrow) with calcification in the midline cerebellum. (b) The mass becomes bright on T2-weighted image, suggesting less compact cellularity. (c) Postcontrast image reveals strong enhancement of the mass. (d) Increased diffusion compared to the normal cerebellar parenchyma is seen on ADC map. (e) Perfusion image (rCBV map) reveals slightly increased perfusion of the cerebellar mass (arrow) compared to the cerebellar hemisphere. (f) Choline/creatinine map obtained from multivoxel proton MRS in 2D array demonstrates increased choline in the tumor
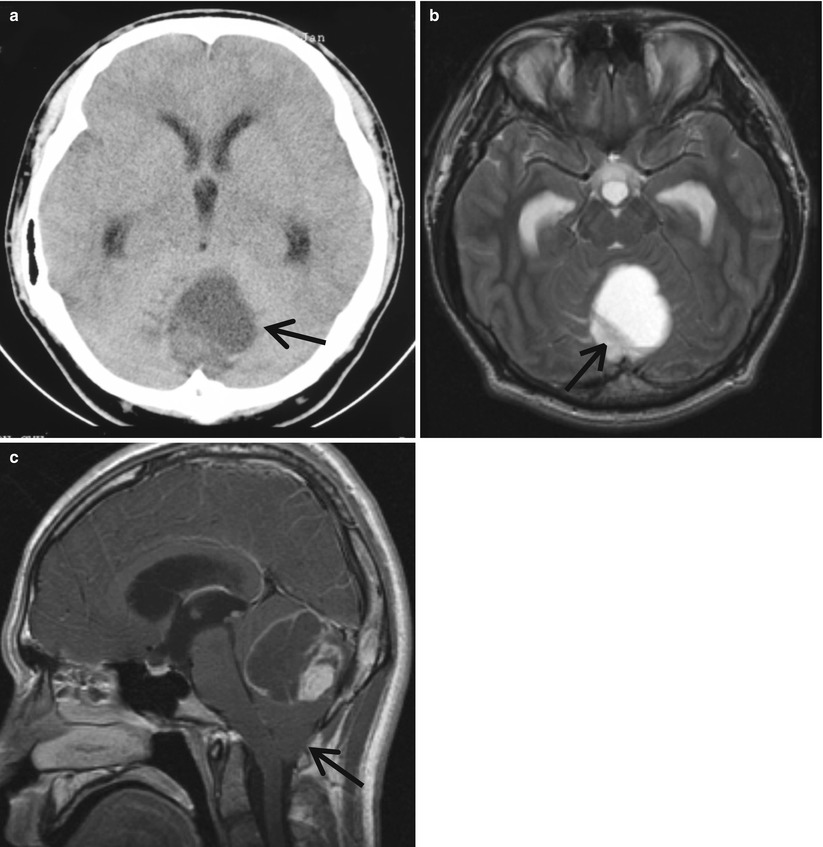
Fig. 4.2
Cystic cerebellar JPA in an 18-year-old boy. (a) CT scan shows cystic mass with solid portion (arrow), which appears low attenuated compared to the normal parenchyma. (b) Solid portion exhibits high intensity on T2-weighted image (arrow). (c) Postcontrast sagittal image reveals strong enhancement of the solid portion and cystic wall. The fourth ventricle is compressed, and the cerebellar tonsil (arrow) is downward-displaced
4.3.1.1.2 Medulloblastomas
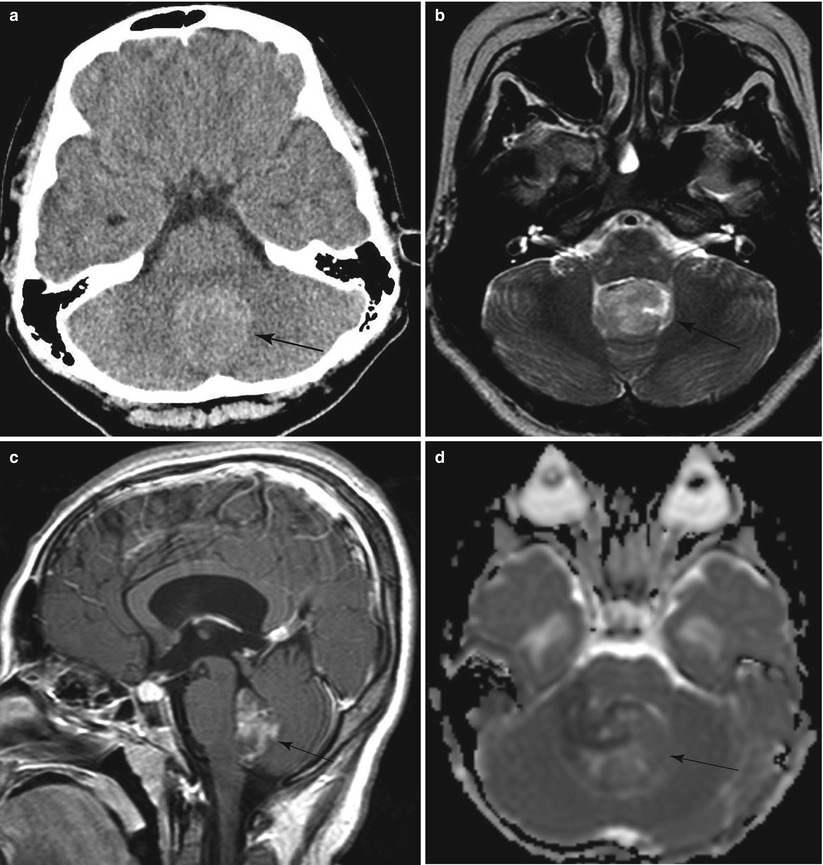
Fig. 4.3
Medulloblastoma in an 11-year-old girl. (a) Noncontrast CT shows hyperdense midline cerebellar mass (arrow). (b) The mass (arrow) shows slight hyperintensity compared to the gray matter on T2-weighted image. (c) Postcontrast sagittal image reveals the mass arising from the roof of the fourth ventricle filling the ventricular lumen (arrow). (d) ADC map demonstrates isointensity to the normal parenchyma (arrow) and more restricted diffusion compared to the JPA in (Fig. 4.1d)
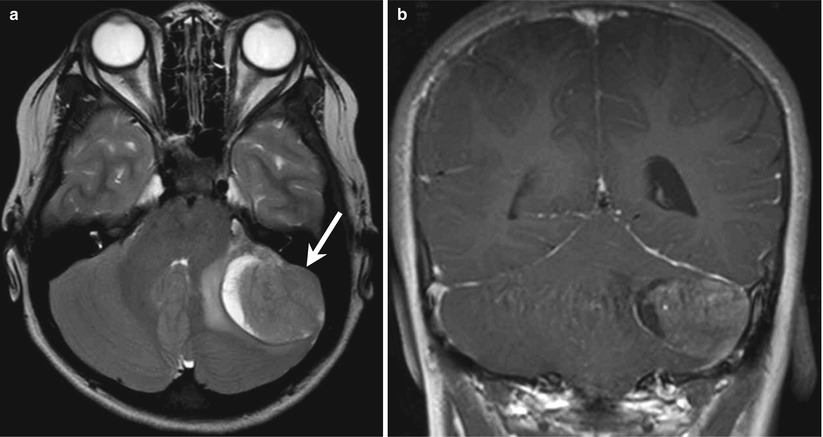
Fig. 4.4
Atypical medulloblastoma in a 16-year-old girl. (a) T2-weighted axial image shows well-defined iso-signal intensity mass (arrow) with peripheral cystic portion and surrounding edema in the left cerebellar hemisphere. (b) Postcontrast coronal image reveals homogeneous enhancement of the solid portion and cyst wall

Fig. 4.5
Medulloblastoma with disseminated tumors in the CSF space. (a) Postcontrast axial image of the brain shows enhancing cerebellar tumor and enhancing lesions (arrows) in both cerebellopontine angles (CPA) and thick sulcal enhancement of both temporal lobes as well as enhancing folia suggesting disseminated tumor. (b) Postcontrast sagittal image of the spine demonstrates extensive enhancing lesions along the spinal cord invading the parenchyma and along the cauda equina. (c) T2-weighted image shows enlarged cord with abnormal intensity and isointensity mass (arrow) in the thecal sac
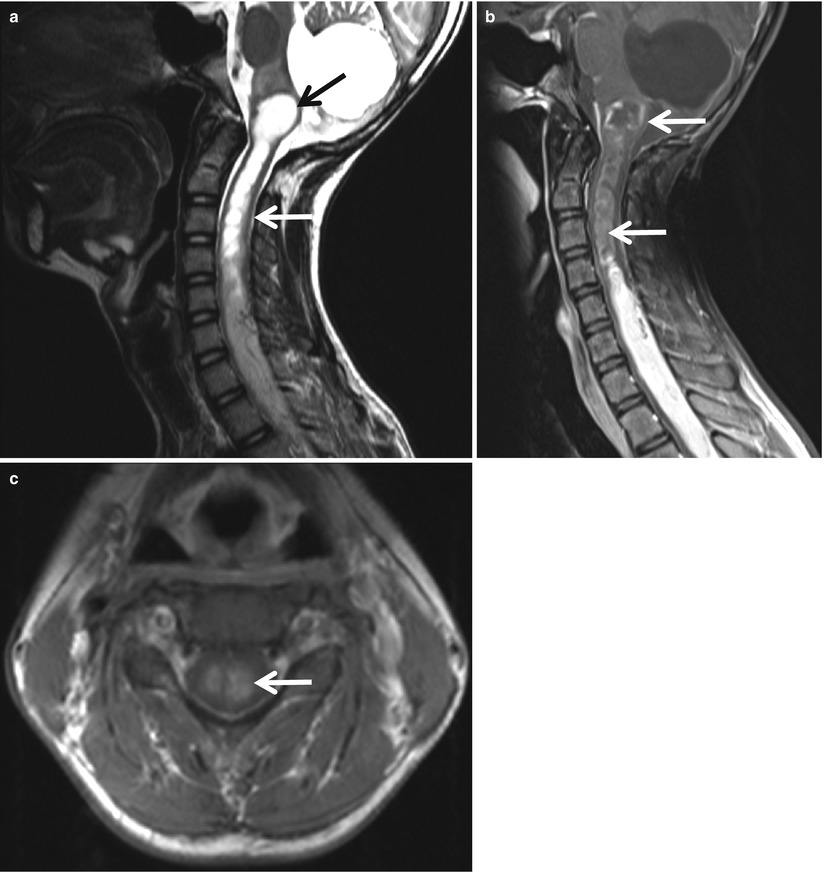
Fig. 4.6
Intramedullary lesion caused by central canal seeding of the medulloblastoma. (a) T2-weighted sagittal image shows hydrosyrinx of the upper cervical cord (white arrows), extending upward to the medulla (arrow) surrounded by edema, and extensive intramedullary masses. Prior surgical defect is seen in the cerebellum. (b) Lining of the cystic lesion in the medulla and hydrosyrinx (arrow), lower solid portions, and distal cord surface are enhanced on a postcontrast sagittal image, suggesting tumor seeding. (c) Enhancing lesion (arrow) is seen at the central portion of the cord on a postcontrast axial image, suggesting tumor seeding through the central canal
4.3.1.1.3 Ependymomas
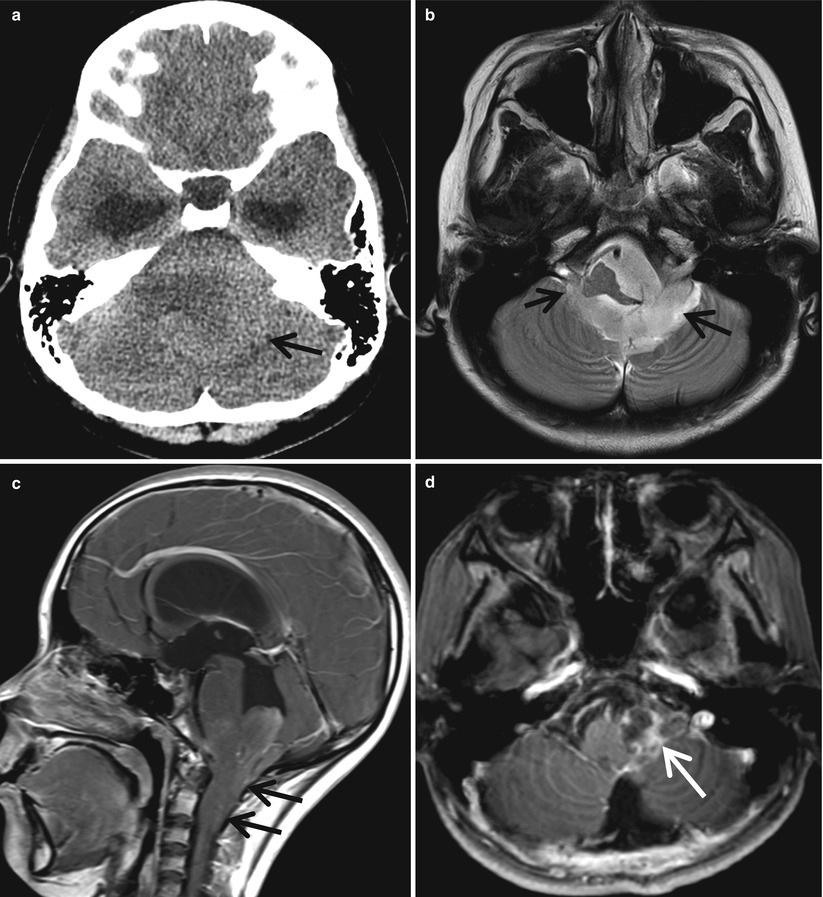
Fig. 4.7
Ependymoma in a 12-year-old girl. (a) CT scan shows isodensity mass in the cerebellum and distended temporal horns, suggesting obstructive hydrocephalus. (b) The mass is occupying the fourth ventricle extending through both the foramen of Luschka (arrow) into the CPA areas. Indentation and displacement of medulla are seen, and the basilar artery is encased. (c) Tongue-like extension of the mass (arrows) is seen through the foramen of Magendie onto the posterior aspect of the upper cervical cord on a postcontrast sagittal image. (d) Postoperative follow-up MR image reveals residual tumor (arrow) in the left CPA
4.3.1.1.4 Brain Stem Tumors
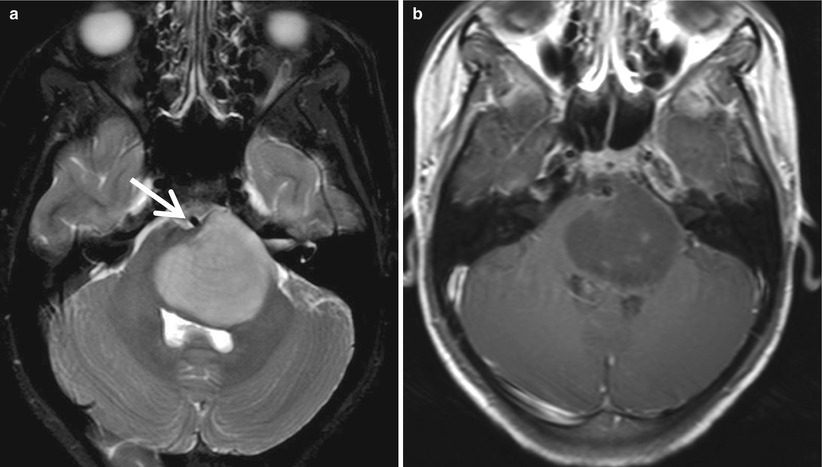
Fig. 4.8
Diffuse pontine glioma. (a) Large pontine mass is seen as high intensity expanding the pons on T2-weighted image. The basilar artery (arrow) is partially engulfed. (b) The mass is not well enhanced on postcontrast image
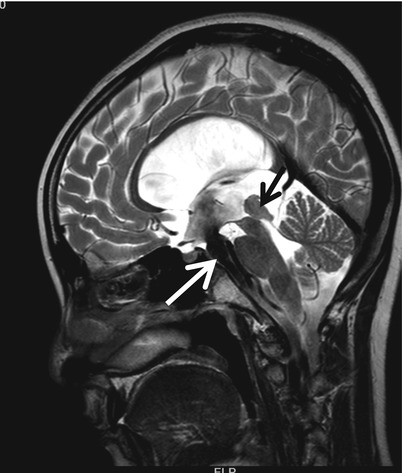
Fig. 4.9
Tectal glioma causing hydrocephalus in a 10-year-old boy who underwent endoscopic third ventriculostomy. T2-weighted sagittal image shows enlarged midbrain tectum (black arrow) causing aqueductal obstruction. Prominent flow artifact is noted (white arrow), suggesting patent defect at the floor of the third ventricle
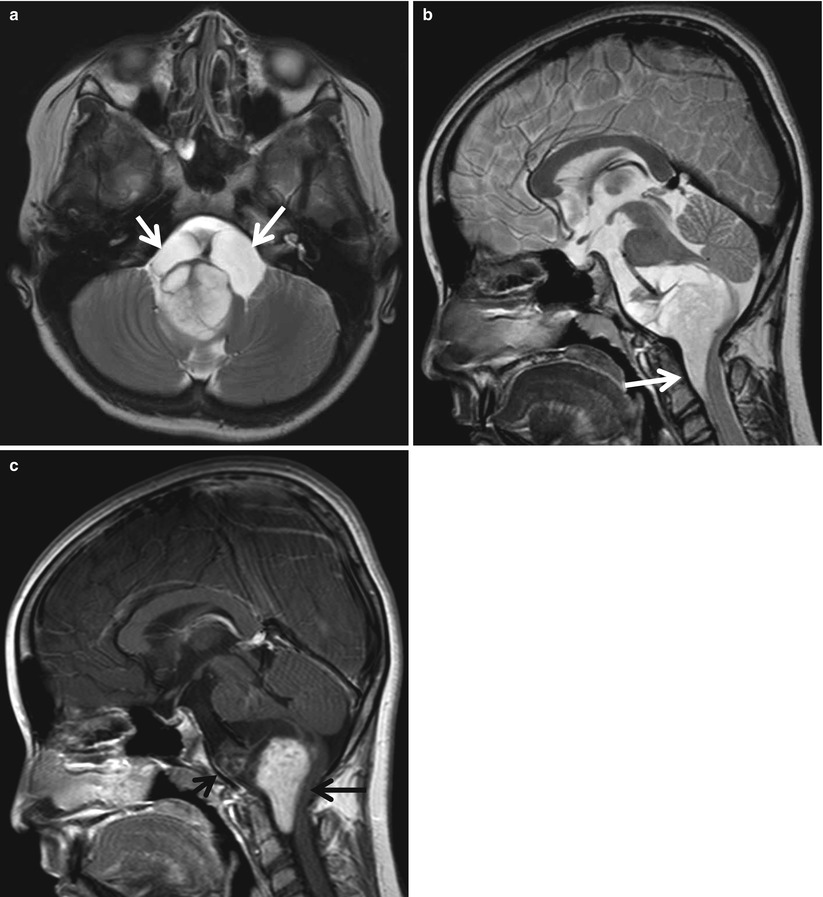
Fig. 4.10
Exophytic JPA involving the medulla in a 15-year-old boy. (a) T2-weighted axial image shows a well-defined solid and cystic mass arising from the medulla. The solid portion is very bright, and cystic portions (arrows) are encasing the basilar artery. (b) The mass is protruded inferiorly anterior to the cervical cord (arrow) and superiorly compressing the pons on T2-weighted sagittal image. (c) The solid portions (arrows) are well enhanced on a postcontrast sagittal image
4.3.1.1.5 Extraparenchymal Tumors
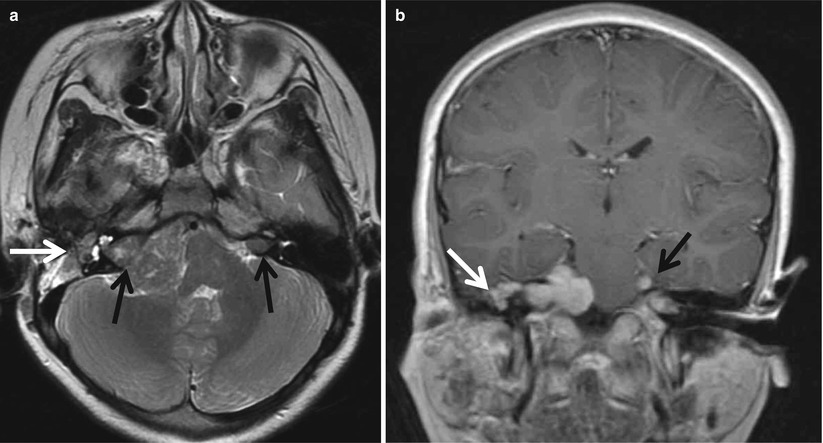
Fig. 4.11
Multiple cranial nerve tumors in patient with type 2 neurofibromatosis. (a) T2-weighted coronal image shows bilateral internal auditory canal masses (black arrows) of isointensity compared to the brain. The right one is extending to the CPA area compressing the pons. Another mass is seen at the right facial nerve location (white arrow). (b) Postcontrast coronal image reveals multiple enhancing tumors involving bilateral acoustic nerves, right facial nerves (white arrow), and left trigeminal nerve (black arrow)
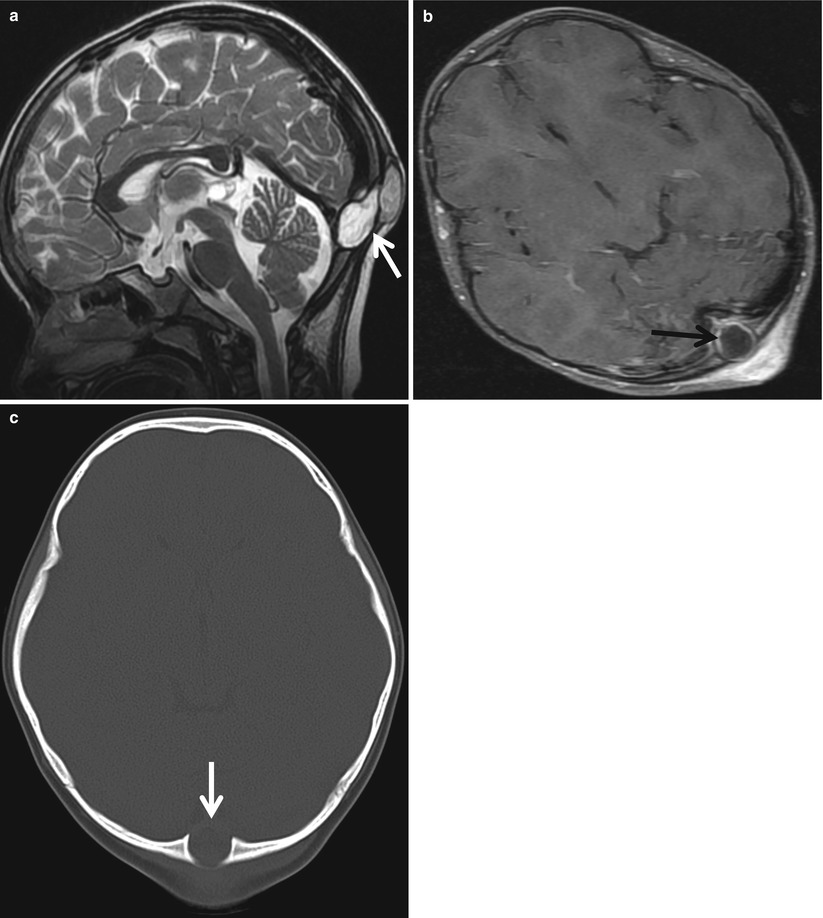
Fig. 4.12
Infected dermoid cyst. (a) T2-weighted sagittal image shows midline posterior cysts (arrow) involving both soft tissue in the scalp and occipital skull. (b) The cystic wall is enhanced (arrow), and more patch enhancement is seen at the adjacent scalp suggesting infection on a postcontrast axial image. (c) CT scan demonstrates well-defined bony defect (arrow) at the occipital bone
4.3.1.2 Cerebral Hemispheric Tumors
4.3.1.2.1 Astrocytomas
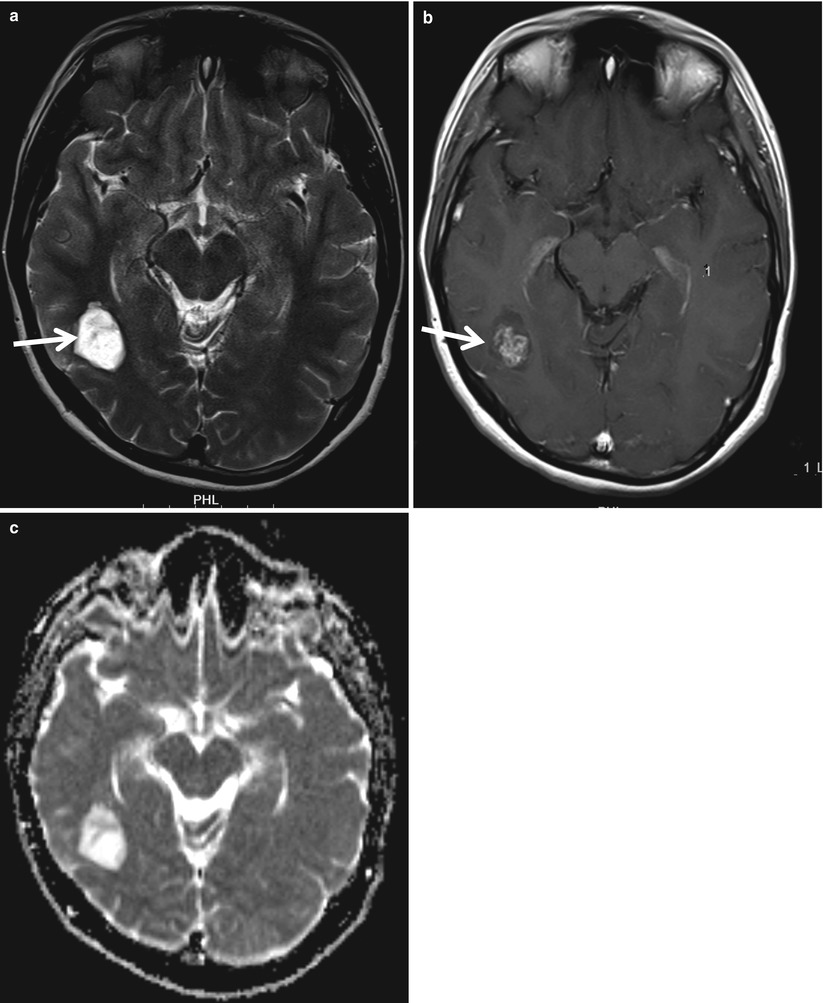
Fig. 4.13
Small hemispheric JPA in a 14-year-old boy. (a) T2-weighted axial image shows well-defined high-intensity mass (arrow) in the right temporo-occipital lobe. (b) The mass is heterogeneously enhanced after contrast administration. (c) Increased ADC is seen on water diffusion map
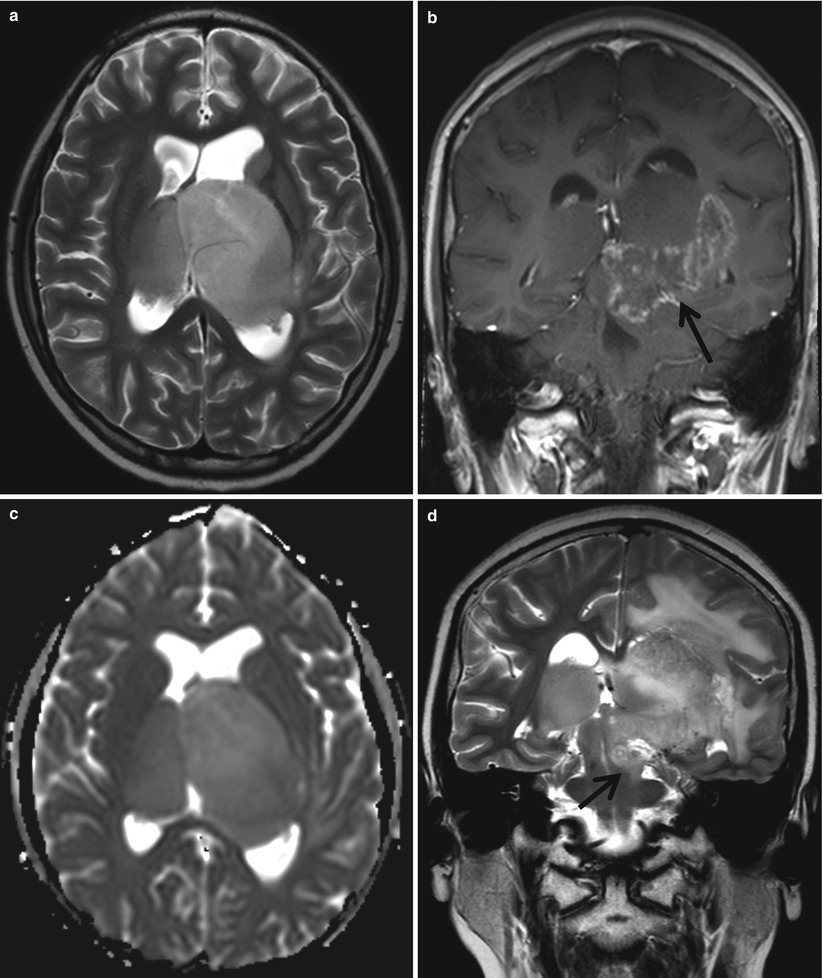
Fig. 4.14
Anaplastic astrocytoma involving bilateral thalami. (a) Bilateral thalamic mass causing enlarged thalami are seen on T2-weighted image. (b) Focal heterogeneous enhancement (arrow) is noted on postcontrast coronal image. (c) The mass exhibits iso-signal intensity of ADC map. (d) Coronal T2-weighted image obtained 7 months later reveals progressed tumor extension into the brain stem (arrow) and extensive peritumoral edema
4.3.1.2.2 Subependymal Giant Cell Astrocytoma
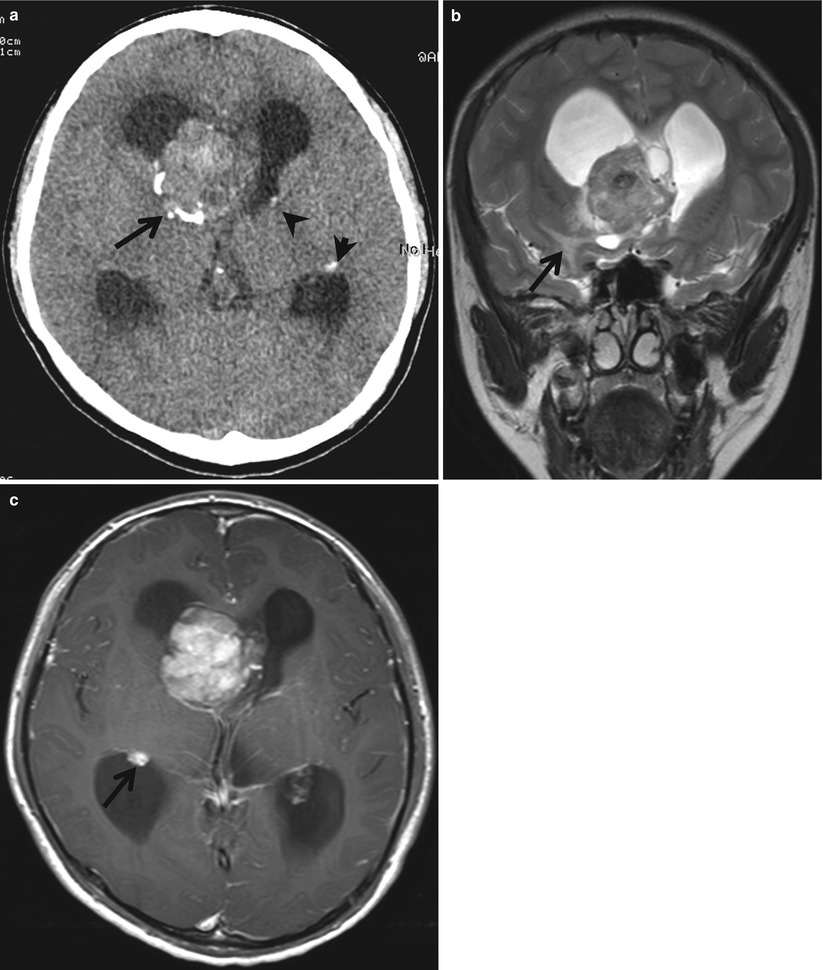
Fig. 4.15
Giant cell astrocytoma in a patient with tuberous sclerosis. (a) Precontrast CT scan shows lobulating mass with calcification (arrow) at the right foramen Monro resulting in ventricular distension. Multiple subependymal calcified nodules are noted (arrowheads), suggesting tuberous sclerosis. (b) The mass shows slightly high intensity, containing dark spots associated with mild peritumoral edema on a T2-weighted coronal image. Focal subcortical high-intensity lesion of adjacent right temporal lobe (arrow) is considered to be a subcortical tuber. (c) Postcontrast axial image shows heterogeneous tumor enhancement. Another small high-intensity subependymal nodule is seen in the right temporal horn (arrow)
4.3.1.2.3 Gangliomas and Gangliocytomas
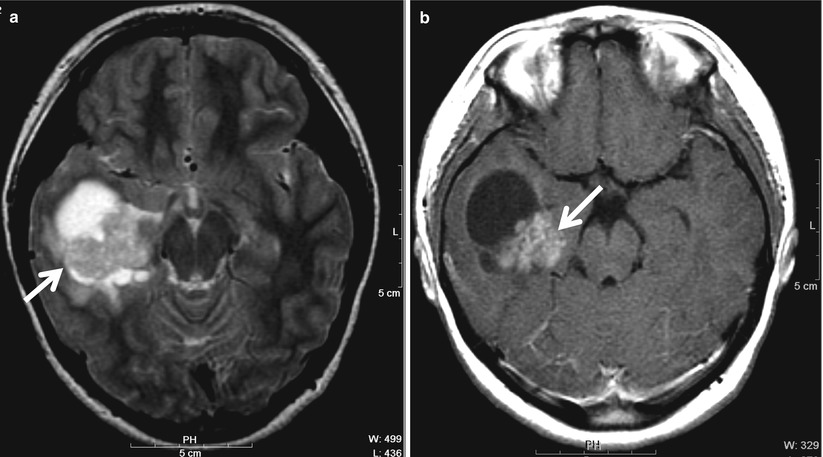
Fig. 4.16
Ganglioglioma in a 13-year-old girl. (a) T2-weighted image shows solid and cystic mass in the right temporal lobe (arrow). (b) The solid portion is heterogeneously enhanced (arrow), surrounded by mild edema on a postcontrast image
4.3.1.2.4 Dysembryoplastic Neuroepithelial Tumors
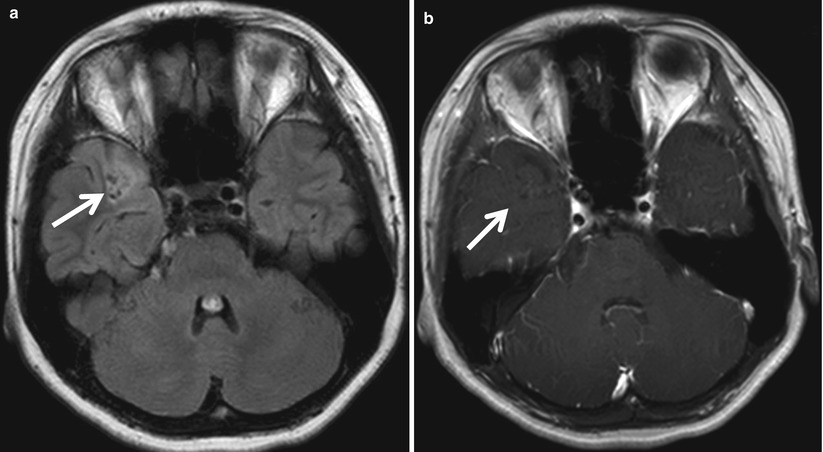
Fig. 4.17
Dysembryoplastic neuroepithelial tumor (DNET) associated with adjacent focal cortical dysplasia in a 14-year-old girl. (a) FLAIR image shows localized high-intensity lesion containing multiple tiny cysts (arrow) in the right temporal lobe. Subtle hyperintensity is also noted at the adjacent cortex. (b) The lesion (arrow) is not enhanced on a postcontrast axial image
4.3.1.2.5 Supratentorial Ependymoma
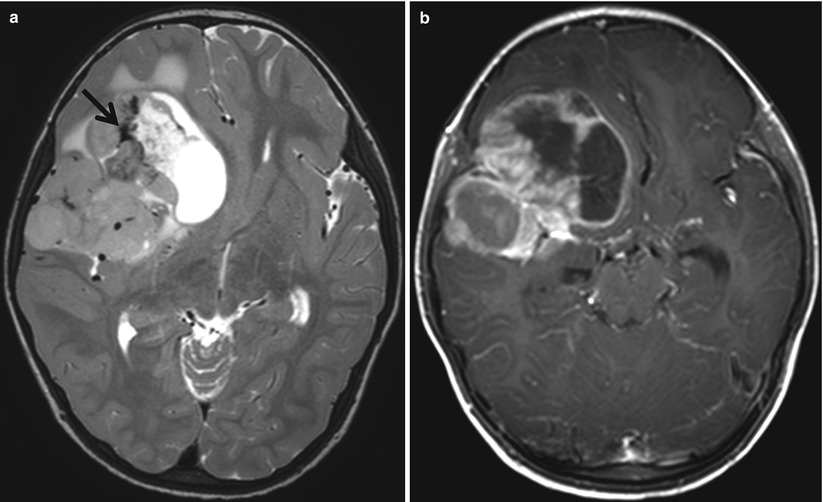
Fig. 4.18




Supratentorial ependymoma in a 3-year-old boy. (a) T2-weighted image shows solid and cystic mass in the right frontotemporal lobe. The mass contains dark intensity (arrow), suggesting calcification, and surrounded by mild edema. (b) The solid portion and cystic wall are enhanced on a postcontrast image
Related posts:



Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
