Chapter 10 Nerves of the lumbar spine
Lumbar spinal nerves
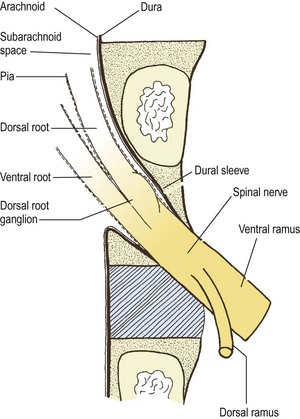
The lumbar spinal nerves lie in the intervertebral foramina and are numbered according the vertebra beneath which they lie. Thus, the L1 spinal nerve lies below the L1 vertebra in the L1–2 intervertebral foramen, the L2 spinal nerve lies below the L2 vertebra, and so on. Centrally, each spinal nerve is connected to the spinal cord by a dorsal and ventral root. Peripherally, each spinal nerve divides into a larger ventral ramus and a smaller dorsal ramus. The spinal nerve roots join the spinal nerve in the intervertebral foramen, and the ventral and dorsal rami are formed just outside the foramen. Consequently, the spinal nerves are quite short. Each is no longer than the width of the intervertebral foramen in which it lies (Fig. 10.1).
Lumbar nerve roots
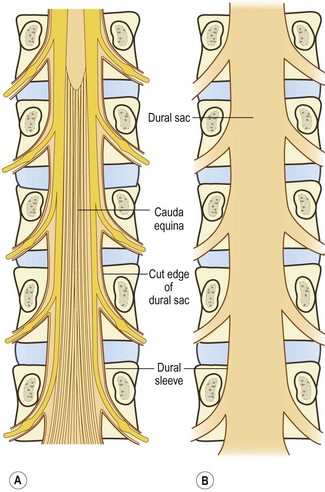
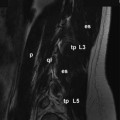
The spinal cord terminates in the vertebral canal opposite the level of the L1–2 intervertebral disc, although it may end as high as T12–L1 or as low as L2–3.1 Consequently, to reach the spinal cord, the lower lumbar (and sacral) nerve roots must run within the vertebral canal where they are largely enclosed in the dural sac (Fig. 10.2). Within the dural sac, the lumbar nerve roots run freely, mixed with the sacral and coccygeal nerve roots to form the cauda equina, and each root is covered with its own sleeve of pia mater, which is continuous with the pia mater of the spinal cord. All the roots of the cauda equina are bathed in cerebrospinal fluid (CSF), which percolates through the subarachnoid space of the dural sac.
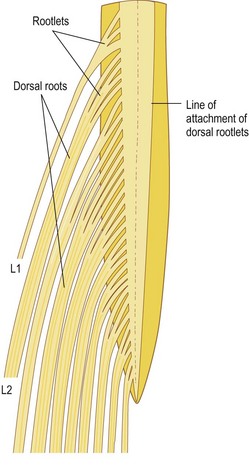
For the greater part of their course, the nerve fibres within each nerve root are gathered into a single trunk, but near the spinal cord they are separated into smaller bundles called rootlets, which eventually attach to the spinal cord. The size and number of rootlets for each nerve root are variable but in general they are 0.5–1 mm in diameter and number between two and 12 for each root.2 The rootlets of each ventral root attach to the ventrolateral aspect of the cord, while those of the dorsal roots attach to the dorsolateral sulcus of the cord, and along the ventral and dorsal surface of the cord the rootlets form an uninterrupted series of attachments (Fig. 10.3).
A pair of spinal nerve roots leaves the dural sac just above the level of each intervertebral foramen. They do so by penetrating the dural sac in an inferolateral direction, taking with them an extension of dura mater and arachnoid mater referred to as the dural sleeve (see Fig. 10.2). This sleeve encloses the nerve roots as far as the intervertebral foramen and spinal nerve, where the dura mater merges with, or becomes, the epineurium of the spinal nerve (see Fig. 10.1). The pia mater of each of the nerve roots also extends as far as the spinal nerve, as does an extension of the subarachnoid space (see Fig. 10.1). Thus, the nerve roots are sheathed with pia mater and bathed in CSF as far as the spinal nerve.
The angle at which each pair of nerve roots leaves the dural sac varies from above downwards. The L1 and L2 roots leave the dural sac at an obtuse angle but the dural sleeves of the lower nerve roots form increasingly acute angles with the lateral margins of the dural sac (see Fig. 10.2). The angles formed by the L1 and L2 roots are about 80° and 70°, respectively, while the angles of the L3 and L4 roots are each about 60°, and that of the L5 roots is 45°.3
The level of origin of the nerve root sleeves also varies from above downwards. In general, the sleeves arise opposite the back of their respective vertebral bodies. Thus, the L1 sleeve arises behind the L1 body, the L2 sleeve behind the L2 body, and so on. However, successively lower sleeves arise increasingly higher behind their vertebral bodies until the sleeve of the L5 nerve roots arises behind the L4–5 intervertebral disc.3
Relations of the nerve roots
The relations of the nerve roots are of critical importance in the pathology of nerve root compression, for space-occupying lesions of any of the tissues intimately, or even distantly, related to the nerve roots may encroach upon them. In this regard, the majority of structures related to the nerve roots have already been described (see Ch. 5), although the anatomy of the spinal blood vessels is described in detail in Chapter 11.
The most intimate relation of the nerve roots are the meninges. The roots of the cauda equina are enclosed in the dural sac and bathed in CSF. Beyond the dural sac, individual pairs of roots are sheathed by pia, arachnoid and dura in the nerve root sleeves (Figs. 10.1, 10.4). The relevance of this relationship is that tumours or cysts of the dura or arachnoid can at times form space-occupying lesions that compress the roots. Running within the root sleeves are the radicular arteries and veins (see Ch. 11), and the relevance of this relationship is described in Chapter 15.
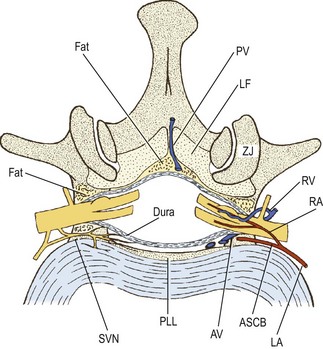
As a whole, the dural sac rests on the floor of the vertebral canal (see Ch. 5). The anterior relations of the dural sac, therefore, are the backs of the vertebral bodies and the intervertebral discs, and covering these structures is the posterior longitudinal ligament (see Fig. 10.4). Running across the floor of the vertebral canal, and therefore anterior to the dural sac, are the anterior spinal canal arteries (see Ch. 11) and the sinuvertebral nerves (see below). Posteriorly, the dural sac is related to the roof of the vertebral canal, the laminae and ligamenta flava (see Ch. 5).
A space intervenes between the dural sac and the osseoligamentous boundaries of the vertebral canal; this space is referred to as the epidural space. This space, however, is quite narrow, for the dural sac is applied very closely to the osseoligamentous boundaries of the vertebral canal. It is almost a ‘potential space’, and the term ‘epidural region’ has been advocated as an alternative description to avoid the connotation of a wide, empty space (see Fig. 10.4).4
The epidural space is principally filled by a thin layer of areolar connective tissue, which varies from diaphanous to pseudomembranous in structure.4 Some investigators, however, consider this to be a substantive structure which they call the epidural membrane.5 The membrane surrounds the dural sac and lines the deep surface of the laminae and pedicles. Ventrally, opposite the vertebral bodies, the membrane lines the back of the vertebral body and then passes medially deep to the posterior longitudinal ligament, where it attaches to the anterior surface of the deep portion of the ligament.5 The membrane does not cover the back of the anulus fibrosus; it is prevented from doing so by the posterior longitudinal ligament as it expands laterally over the back of the disc. Consequently, the membrane blends with the upper and lower borders of the anulus fibrosus but in a plane just anterior to that of the posterior longitudinal ligament. Opposite the intervertebral foramen, the membrane is drawn laterally to form a circumneural sheath around the dural sleeve of the nerve roots and spinal nerve.5
Running within the areolar tissue of the epidural membrane are the anterior and posterior internal vertebral venous plexuses (see Ch. 11), and located within it are collections of fat. The epidural fat is not distributed uniformly throughout the epidural space but is concentrated around the nerve roots in the intervertebral foramina and in collections wrapped in areolar tissue and lodged in the midline recesses between the ligamenta flava at each segmental level.4
Within the vertebral canal, the dural sac and the nerve root sleeves are tethered to the vertebral column by condensations of the epidural fascia that have been referred to as dural ligaments or meningovertebral ligaments or the ligaments of Hofmann.4,6–8 Although the first term is the more traditional, the second is a better description, in that the tissue is not an extension of dura but a connection between the meninges and the vertebral column.
The ventral meningovertebral ligaments pass from the ventral surface of the dura to the posterior longitudinal ligament. They are most evident when the dura is drawn backwards and the ligaments are tensed. At rest, they are barely distinguishable from the epidural membrane. When tensed, they form a discontinuous septum in the median or paramedian plane. Individual ligaments may form single bands, bands that bifurcate in a Y shape towards the posterior longitudinal ligament, or two or more paramedian bands that skirt the posterior longitudinal ligament and attach to the periosteum of the lateral recesses.6,7 These ligaments are variably developed at the L1–L4 levels but are well developed at L5.8
Lateral meningovertebral ligaments pass from the lateral surface of the dural sac to blend with the periosteum of the pedicles and with the capsule of the zygapophysial joint.6 Posteriorly, the dural sac is attached to the roof of the vertebral canal by occasional, weak pseudoligamentous connections,4 which represent dorsal meningovertebral ligaments.6
The nerve root sleeves are tethered both within the vertebral canal and in the intervertebral foramen. At the proximal end of the root sleeve, the meningovertebral ligaments tether the dura to the posterior longitudinal ligament and the periosteum of the adjacent pedicle.8,9 In the intervertebral foramen, the root sleeve is surrounded by the circumneural sheath, which indirectly binds the nerve roots and spinal nerve to the margins of the foramen, but mainly to the capsule of the zygapophysial joint dorsally.8,9 At the outer end of the intervertebral foramen, the spinal nerve may be related to a transforaminal ligament when one is present (see Ch. 4). As a rule, the spinal nerve lies below most forms of transforaminal ligaments but emerges above the inferior transforaminal variety (see Ch. 4).10
The relative size of the spinal nerve and nerve roots within the intervertebral foramen varies from level to level and is important with respect to the risk of spinal nerve and nerve root compression. As an approximate rule, the cross-sectional area of an intervertebral foramen increases from L1–2 to L4–5, but the L5–S1 foramen is conspicuously smaller than the rest,11 yet, paradoxically, the L5 spinal nerve is the largest of the lumbar nerves.11 Consequently, the L5 spinal nerve occupies about 25–30% of the available area in an intervertebral foramen, while the other lumbar nerves occupy between 7% and 22%, making the L5 nerve the most susceptible to foraminal stenosis.
Anomalies of the nerve roots
The clinically most significant anomalies of the lumbar nerve roots are aberrant courses and anastomoses between nerve roots;12–18 the morphology of these anomalies is summarised in Figure 10.5.
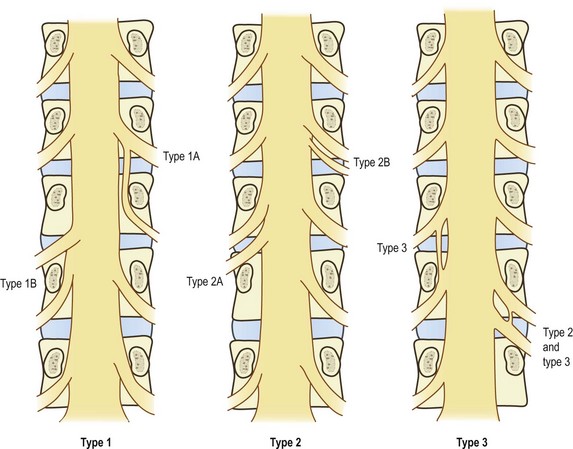
Fortunately, symptomatic nerve root anomalies are not common, and such confusing considerations do not regularly complicate clinical practice. The incidence of anomalies has been estimated at about 8.5%,19 but when symptomatic the major types are readily recognised in myelograms.2 Nonetheless, nerve root anomalies should be borne in mind and considered as a possibility in patients with unusual distributions of neurological signs.
The surgical significance of nerve root anomalies relates to the mobility of anomalous nerve roots, the care necessary when operating in their vicinity, and the types of procedures that can be carried out to decompress them. These issues are explored in the surgical literature.2,16
Another feature of nerve roots, which is not an anomaly but rather a variation, is intrathecal anastomoses. Within the dural sac, bundles of nerve fibres may pass from one nerve root to the next, and such communications have an incidence of 11–30%.20 They usually occur close to the spinal cord and may vary in size from small filaments to substantial bundles.20 Since they occur proximal to the regions where nerve roots are liable to compression, these anastomoses are not of diagnostic clinical significance, but they are of relevance to neurosurgeons operating on the proximal ends of nerve roots.20,21
Dorsal rami
The L1– L4 dorsal rami are short nerves that arise almost at right angles from the lumbar spinal nerves.22 Each nerve measures about 5 mm in length23 and is directed backwards towards the upper border of the subjacent transverse process. The L5 dorsal ramus differs, in that it is longer and travels over the top of the ala of the sacrum (Fig. 10.6).23
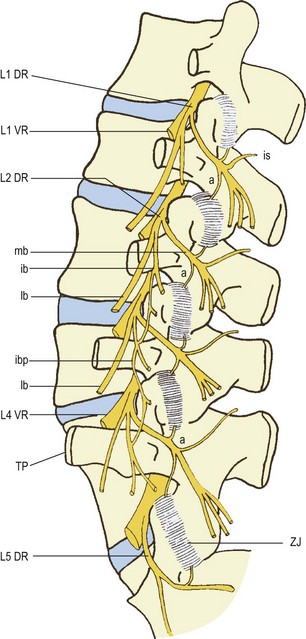
Figure 10.6 A left posterior view of the lumbar spine showing the branches of the lumbar dorsal rami. (Based on Bogduk et al. 1982.23) DR, dorsal ramus: ib, intermediate branch; ibp, intermediate branch plexus; lb, lateral branch; mb, medial branch. TP, transverse process; a, articular branch; is, interspinous branch. VR, ventral ramus. ZJ, zygapophysial joint.
As they approach their transverse processes, the L1–4 dorsal rami divide into two or three branches (see Fig. 10.6). A medial branch and a lateral branch are always represented at every level. The variable, third branch is the intermediate branch. Although this branch is always represented, it frequently arises from the lateral branch instead of the dorsal ramus itself.23


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


