Axial skeleton
Appendicular skeleton
Chest (AP, lateral, and bilateral obliques to include the upper lumbar spine
Humeri (AP)
Pelvis (AP), to include the mid-lumbar spine
Forearms (AP)
Lumbosacral spine (lateral)
Femurs (AP)
Cervical spine (AP and lateral)
Lower legs (AP)
Skull (frontal and lateral)
Hands and feet (AP)
The babygram, which is a single image of the entire chest and abdomen as well as the extremities, is inadequate. Peripheral areas are incorrectly exposed, and subtle fractures can be missed. Proper radiographic technique, positioning, collimation, and shielding are vital to optimize visualization of osseous structures and allow diagnosis of pathology with high sensitivity while keeping radiation dose levels within acceptable limits. A follow-up skeletal survey, usually in 2 weeks, may increase the diagnostic yield, particularly if findings are equivocal on the initial study and there is strong clinical suspicion for abuse. The repeat study also helps with accurate dating of individual injuries.
Although the complete skeletal survey is almost always mandatory in suspected child abuse cases for patients under 2 years of age, its utility diminishes and provides little value after age 5. Between the ages of 2 and 5 years, imaging is guided by specific clinical indicators of abuse and should be individually prescribed [10].
Bone scintigraphy is generally limited in the evaluation of non-accidental injury. Its primary use is in the identification of subtle rib fractures, but it is not particularly good at demonstrating epiphyseal and metaphyseal fractures, as these areas are obscured by normal physiologic activity and high periphyseal uptake of radiopharmaceutical [11]. Skull fractures are notoriously difficult to visualize on routine bone scans [12]. Equally important, bone scans require sedation and expose the child to a relative high radiation dose [13]. They are mainly used if clinical suspicion is high and routine imaging fails to document acute or healing fractures.
There has been recent interest in computed tomography (CT) for initial imaging of rib fractures, especially if routine skeletal survey fails to document fractures in highly suspicious cases [14]. Magnetic resonance imaging is very sensitive for evaluating spine, pelvis, and long bone occult skeletal trauma in children [15] but is limited for evaluating rib and skull fractures. It may not show classic metaphyseal lesions [16]. Ultrasonography can be valuable for assessing epiphyseal separations that are suspected on routine radiographs. However, its operator dependence, lack of correlative data for dating fractures, and limited utility for follow-up imaging make it the least useful modality for evaluating non-accidental trauma.
2 Fracture Patterns
The classification of fractures into high, moderate, and low specificity for child abuse is well established (Box 18.1). High-specificity injuries include the classic metaphyseal lesion (CML) and rib, scapular, sternal, and spinous process fractures. Moderately specific fractures include multiple and/or bilateral fractures of varying ages and vertebral, digital, and complex skull fractures. Long bone diaphyseal fractures as well as clavicular and linear skull fractures are considered low-specificity injuries [17].
Box 18.1: Specificity of Skeletal Fractures
Specificity | Types of fractures |
|---|---|
High | Classic metaphyseal lesions (CML)/corner fractures |
Rib fractures, especially posteromedial | |
Scapular fractures | |
Sternal fractures | |
Multiple fractures of varying ages | |
Vertebral body fractures | |
Digital fractures | |
Complex skull fractures | |
Low | Linear skull fractures |
Clavicular fractures | |
Long bone shaft fractures especially in ambulatory children |
2.1 Classic Metaphyseal Lesions (CML)
The terms “corner fracture” and “bucket handle fracture” describe fractures at the metaphyses of the long bones that are highly specific for non-accidental trauma, since nonambulatory children cannot inflict this type of injury on themselves (Box 18.2). The fractures result from tractional and torsional force applied to an extremity and are virtually diagnostic of child abuse, particularly in children under 1 year of age. Violent shaking of an infant causes tearing and injury at the level of the zone of provisional calcification of the physis; the detached bone creates a curvilinear density that constitutes the bucket handle fracture [11] (Fig. 18.1). If this fragment is viewed in tangent, it appears as a detached corner, whereas if it is viewed partially en face it appears as a bucket handle. CMLs involve the metaphyses of long bones and are most common at the proximal or distal tibias, distal femurs, and proximal humeri; they are frequently bilateral [18]. They usually involve the posteromedial aspect of the distal femurs, proximal tibias, and distal tibias. At the proximal humeri, they are usually lateral and are best seen with external rotation.

Fig. 18.1
Classic metaphyseal lesions (CML) showing bucket handle configuration at the distal tibia and fibula (arrows)
Box 18.2: Corner Metaphyseal Lesions
Traction/torsion cause tearing at zone of provisional calcification |
Bucket handle vs. corner fragment appearance results from difference in projection |
Most common: proximal/distal tibias, distal femurs, proximal humeri |
Posteromedial: tibia, femur |
Lateral: humeri |
Differential: birth trauma, orthopedic manipulation, normal metaphyseal spur |
Rarely, a similar lesion may result from birth trauma [19] or from manipulation during orthopedic procedures. The timing of injury and the clinical history differentiate such fractures from abusive trauma. These fractures should also be differentiated from the normal subperiosteal bone collar and normal metaphyseal spur seen in rapidly growing long bones of young children, which are attached to the adjacent bone with no intervening lucency (Fig. 18.2) (see Chap. 2).
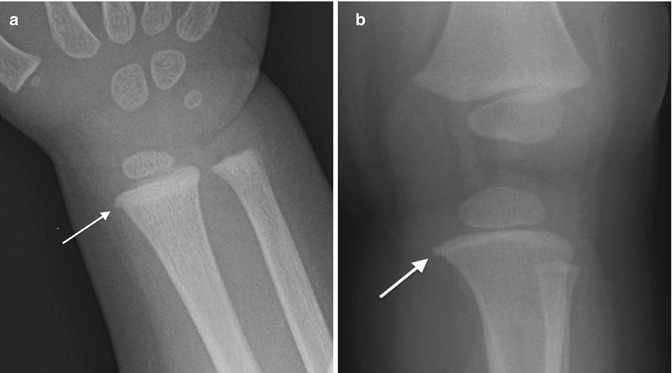

Fig. 18.2
Normal metaphyseal spurs and collars, contrasted with corner fracture. No lucency separates the metaphysis from the normal bone collar (arrows) at the distal radius (a) and proximal tibia (b), or the normal distal femoral spur (arrow, c). (d) Lucency separates the CML (with corner fracture configuration) (arrow) from the metaphysis
2.2 Rib Fractures
Rib fractures are the most common and highly specific injury found in abused children, with positive predictive values as high as 95 % in children less than 3 years of age [18]. Furthermore, in some patients, rib fractures are the only skeletal manifestation of child abuse. Although involvement can be anywhere along the rib, unilateral, bilateral, or multiple posteromedial rib fractures are most specific for child abuse (Fig. 18.3). This is in keeping with the mechanism of how these fractures are sustained when the chest is squeezed in the anteroposterior direction, levering the posteromedial ribs against the transverse processes. For similar fractures to occur in the setting of accidental trauma, massive forces must be generated, such as in deceleration dashboard injuries or high-velocity vehicular impact. Cardiopulmonary resuscitation does not cause posteromedial rib fractures [20].

Fig. 18.3
Healing posteromedial rib fractures at almost every level are highly suggestive of child abuse (arrows indicate two of the many fractures). Multiple posterolateral rib fractures as well
Routine chest radiography may not clearly demonstrate rib fractures, particularly if they are acute, incomplete, and non-displaced or if they are posterior. For this reason, oblique views, follow-up imaging after 2 weeks, and bone scintigraphy have been suggested to improve detection of such fractures. CT of the chest has also been advocated in highly suspicious situations [14] (Fig. 18.4).
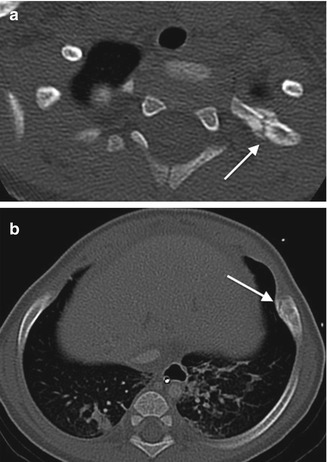
Fig. 18.4
Healing rib fractures on CT. (a) Axial CT shows healing second rib fracture that was not evident on contemporaneous radiograph. (b) Axial CT of a different patient with a healing left anterior rib fracture not evident even on oblique views (arrow)
2.3 Skull Fractures
Skull fractures are common in both accidental and non-accidental injury and are therefore low-specificity lesions. Linear skull fractures occur most frequently, usually upon impact after low-velocity falls. However, complex fractures (such as concentric, star-shaped, or eggshell fractures) imply high-velocity/high-energy trauma and carry a higher positive predictive value for abuse [21, 22] (Fig. 18.5).
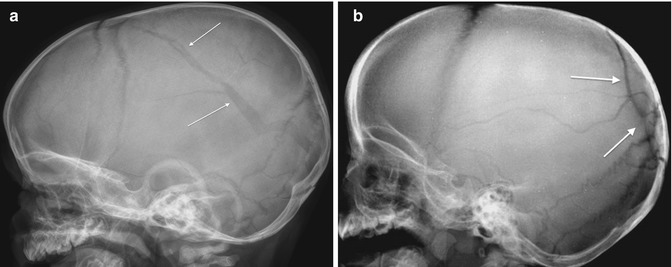
Fig. 18.5
Skull fractures. (a) Linear fracture of the parietal and occipital bones (arrows), a nonspecific fracture that can be accidental or result from abuse. However, diastasis, vague tangential fracture lines, and the fact that the fracture crosses a suture, all features that are less common in the typical fall from a low-height accidental injury, increase the suspicion for abuse. (b) Complex, star-shaped/eggshell fracture (arrows) of the parieto-occipital region indicates a high-impact injury, highly suggestive of abuse
A skull fracture is often the only evidence of abuse. It is therefore important that even these low-specificity lesions are accurately identified and correlated with the clinical history and reported mechanism of injury. This can sometimes present difficulties, especially in subtle cases, where the complex development of the infantile skull may make it difficult to differentiate between a linear fracture and an accessory suture. CT with three-dimensional (3D) reconstruction is very helpful in evaluating a suspicious fracture. Characteristics which favor fracture include a sharp lucency with non-sclerotic edges, fracture line widening as it approaches a suture, and associated soft tissue swelling [23] (Fig. 18.6).
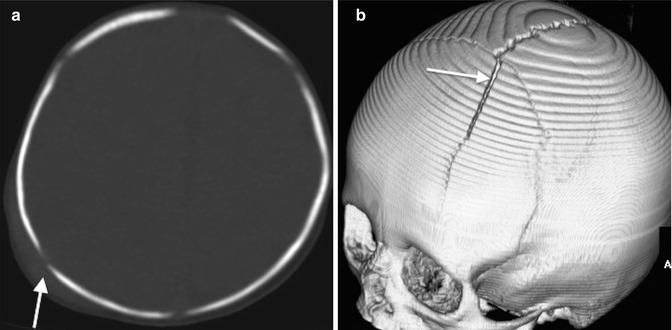
Fig. 18.6
Differentiating skull fractures from accessory cranial sutures. (a) Axial CT shows soft tissue swelling and step-off, which indicate that the lucency in the occipital bone represents fracture (arrow). (b) Three-dimensional CT reconstruction shows a linear lucency in the frontal bone which widens as it approaches the sagittal suture (arrow), also a feature of skull fracture
2.4 Long Bone Diaphyseal Fractures
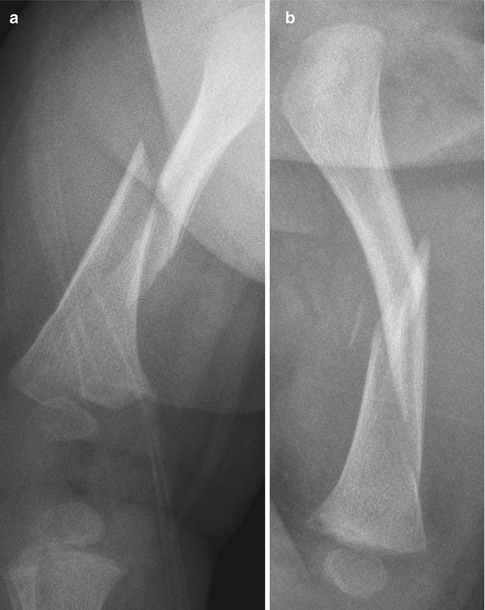
The presence of long bone diaphyseal fractures in a nonambulatory infant should raise concern for non-accidental injury. Such fractures usually result from application of a bending or rotational force, as the extremity is grabbed [22].
However, in older children, long bone fractures usually result from accidental trauma. These fractures are therefore generally of low specificity for abuse. Although spiral midshaft fractures have long been associated with abuse, more recent studies have concluded that the type (spiral, transverse, or oblique) as well as the location of the fracture (diaphyseal or metaphyseal) does not necessarily differentiate accidental from abusive injury. Given the appropriate mechanism of injury, these fracture types can occur in the setting of accidental trauma [24, 25].
2.5 Fractures in Unusual Sites
Fractures from child abuse have been described in virtually every bone [4]. However, spine fractures in the absence of documented high-energy trauma are rare in childhood and should suggest abuse. Mechanisms include hyperextension, hyperflexion, and/or axial loading from violent shaking, deliberate dropping, or throwing. Injury usually involves multiple vertebral levels, often near the thoracolumbar junction (see Chap. 4). Spinous process fractures, as well as vertebral body compression fractures with associated endplate defects, may be seen [26].
Other unusual fracture sites in infants and toddlers include the scapula (Fig. 18.7), sternum, phalanges, metacarpals, metatarsals, and pelvis. Fractures in these locations should also raise the possibility of non-accidental trauma, unless there is a legitimate history of an unusual mechanism of injury. Clavicular fractures—especially involving the middle third—are common and thus in general low-specificity lesions. They may also result from birth trauma but should be attributed to birth only if callus is apparent by age 11 days [11].
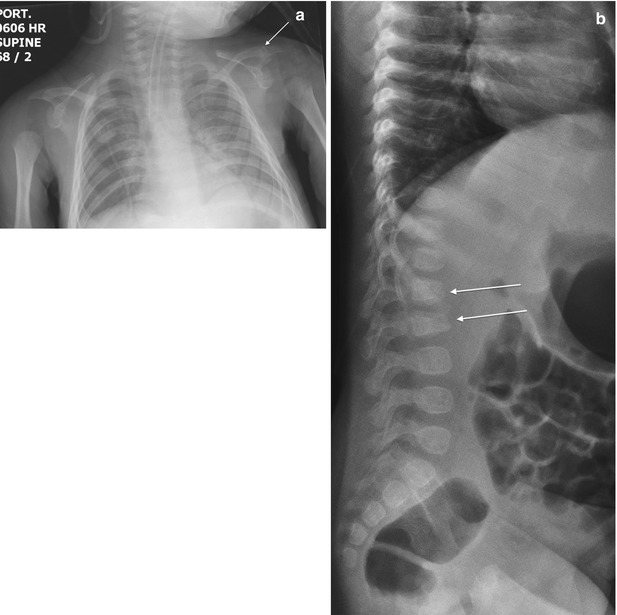
Fig. 18.7
Unusual fractures with high specificity for abuse. (a) Left acromion fracture (arrow), often a result of either non-accidental trauma or high-impact injury. (b) Lumbar vertebral body fractures (arrows) in a nonambulatory infant
2.6 Multiple Fractures of Varying Ages
The presence of multiple fractures without a convincing history of accidental trauma should also raise suspicion for child abuse. There is a significant association between multiple unexplained fractures and child abuse: up to 74 % of abused children have two or more fractures [27]. Bilateral, symmetrical fractures involving the upper or lower extremities in non-ambulatory children are also associated with child abuse (Fig. 18.8).