Normal Anatomic Variants and Miscellaneous Skeletal Anomalies
Lee F. Rogers
L. F. Rogers: Department of Radiology, Wake Forest University School of Medicine, Winston-Salem, North Carolina 27157.
Unlike the congenital and genetic disorders described in Chapter 9, the anatomic variants and miscellaneous skeletal anomalies described here are encountered daily in the practice of radiology. A general familiarity with these structures and their variants is necessary to lessen concern, decrease confusion, and increase the accuracy and confidence of radiographic interpretation. Their importance lies in the fact that they can easily be misinterpreted as pathologic conditions by those unfamiliar with them, when in reality they are of little or no clinical significance. When misconstrued as an abnormality they may lead to costly and unnecessary additional examinations. One of the principal differences between the trained and experienced diagnostic radiologist and other physicians is the ability of the radiologist to recognize and dismiss normal variations, thereby avoiding a potentially expensive, added workup for the patient. The texts by Keats9 and by Kohler and Zimmer11 are excellent, thorough references devoted to this subject. It is difficult to conceive of practicing radiology without one or both of them close at hand. In this chapter, only the most common variants of the peripheral skeleton are described. Many are found in the skull and spine and are covered in Chapters 11 and 12, respectively.
Miscellaneous skeletal anomalies are isolated, anomalous developments. In most cases, they are sporadic and nonfamilial. They may be considered as (1) supernumerary developments, (2) a failure to develop, or (3) segmentation defects.
Supernumerary development is usually seen in the hands and feet as the development of an extra digit (polydactyly) on either side of the hand or foot (Fig. 8-1). These may be sporadic or genetically determined and, at times, are associated with malformation syndromes.
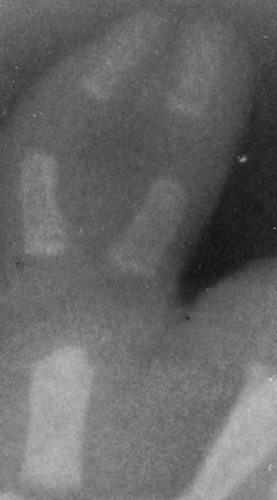 FIG. 8-1. Duplication of the thumb in the newborn. Note the two separate and distinct distal and proximal phalanges, with fusion of the intervening soft tissues. |
Failure to develop is usually either hypoplasia of a structure or, less commonly, aplasia. Hypoplasia is most commonly identified in the middle phalanx of the fifth digit and is known as clinodactyly (Fig. 8-2). This condition may be sporadic, familial, or associated with a whole host of congenital disorders. Hypoplasia and aplasia are most commonly encountered in the posterior elements of the spine, particularly in the pedicle and transverse process.
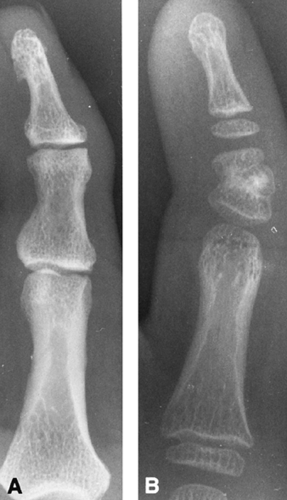 FIG. 8-2. Clinodactyly in a 53-year-old father (A) and his 9-year-old son (B), an example of familial hypoplasia. The deformity was bilateral in both father and son. A: The middle phalanx of the fifth digit is slightly shortened and curved inward. B: The middle phalanx of the fifth digit is short and curved inward distally. The proximal epiphysis of the phalanx is already beginning to close. Compare with the epiphyses of the distal and proximal phalanges. |
Defects of segmentation are common. They may consist of a fusion of segments, commonly encountered in the vertebrae as a partial or complete fusion of two or more vertebral bodies, which is described in Chapter 12. Fusion occurs less commonly in the carpal (Fig. 8-3) and tarsal bones. The fusion of tarsal bones is often symptomatic (Fig. 8-39 and 8-40).
 FIG. 8-3. Lunatotriquetral fusion in a 13-year-old girl. The lunate (L) and triquetrum (T) are fused, and there is a small, incomplete cleft between them distally. |
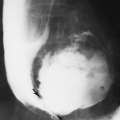
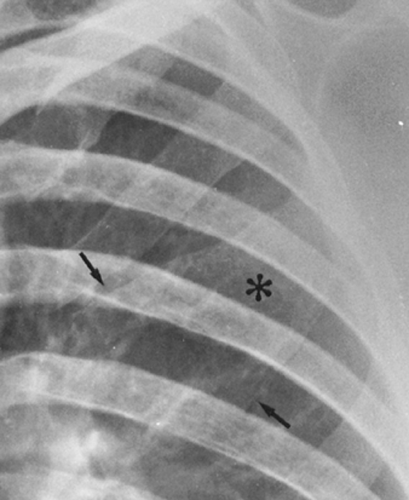 FIG. 8-4. Bifid anterior third anterior left rib (asterisk and arrows). |
 FIG. 8-5. The os tibiale externum (arrow), adjacent to the proximal pole of the navicular. |
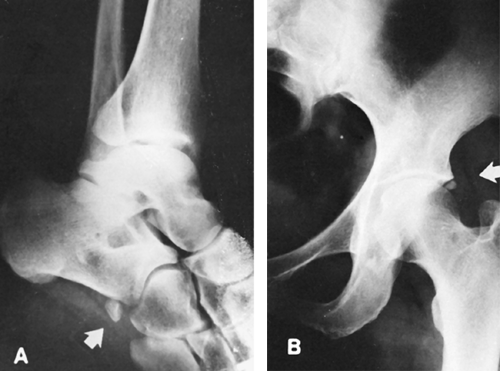 FIG. 8-6. Two accessory ossicles. A: Os peroneum. B: Os acetabuli. |
 FIG. 8-7. Common accessory ossicles in the foot. 1, Os trigonum; 2, os tibiale externum; 3, os peroneum; 4, os intermetatarseum; 5, calcaneus secondarius; 6, supranavicular; 7, secondary astragalus; 8, os vesalianum; 10, os sustentaculi; 12, sesamoid tibiale anterius; S, sesamoid bones. The small black dots over the metatarsal heads and proximal phalanges of first and second toes represent the most frequently observed sites of the sesamoid bones, but they may occur in other locations. There are no numbers 9 or 11 in this diagram. |
 FIG. 8-8. Sesamoid bones. A: Feet. Sesamoid bones underlie the head of each metatarsal (arrows). There are two sesamoids on the great toe, a medial (tibial) sesamoid, and a lateral (fibular) sesamoid. The tibial sesamoid of the great toe and that of the second metatarsal are bifid, a common normal variant. Sesamoid bones are always present on the great toe and less commonly on the fifth. They are rarely encountered on the second, third, and fourth. Although the findings in this case are unusual, they are of no clinical significance. B: Hands. Sesamoid bones are found in relation to the heads of the first, second, and fifth metacarpals (arrows). There is also a sesamoid at the base of the distal phalanx of the thumb (arrow). There are two sesamoids at the head of the first metacarpal. Sesamoid bones of the hand and feet lie within the anterior joint capsule. |
 FIG. 8-9. Lateral view of the proximal femur demonstrating a vascular groove in the posterior cortex (arrow). Note the slightly roughened but normal posterior surface of the cortex. This is known as the linea aspera and represents the site of insertion of the abductor muscles. |
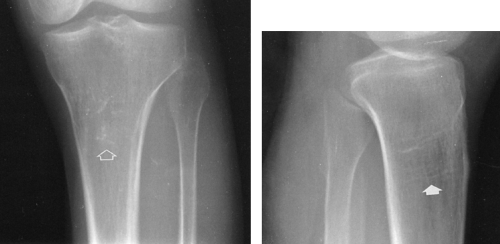 FIG. 8-10. Bone bars. A: Anteroposterior (AP) view. The bright dots (arrow) of trabecular bone are even more dense than the cortex. This is a normal finding and should not be mistaken for evidence of bone infarction or chondroid calcification associated with an endochondroma. B: Lateral view. The bright dots on the AP view are these elongated, horizontal, coarse trabeculae (arrow) seen on end. These are more commonly found in the osteopenic elderly at this site, the distal humerus, and elsewhere. |
 FIG. 8-11. Student’s tumor. Prominent ossification in the cartilaginous ends of the first ribs (arrow). These are easily misconstrued as tumors in the underlying lung. |
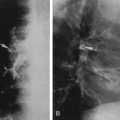
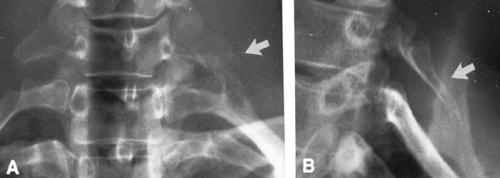 FIG. 8-12. Cervical rib. A: The transverse process of C7 is usually prominent, as seen in this case on the right. The cervical rib extends from this transverse process in a manner similar to the thoracic ribs, as seen on the left (arrow). B: The cervical rib is better seen in the oblique view (arrow). |
 FIG. 8-13. Hypoplastic first ribs. The first rib is hypoplastic bilaterally (arrows). It is often difficult to determine whether there is a hypoplastic first rib or a cervical rib. The distinction is made by simply counting the ribs on both sides. |
 FIG. 8-14. Fusion of the first and second ribs bilaterally (arrows). |
 FIG. 8-15. Ununited apophyses of the transverse processes of L1. The transverse processes are not united with the main body of the vertebra (arrows). Note that the medial borders of the transverse processes are slightly rounded and faintly sclerotic, as are the opposing margins of the base of the transverse processes. The sclerotic margin distinguishes this condition from a fracture. These may be either unilateral or bilateral. |
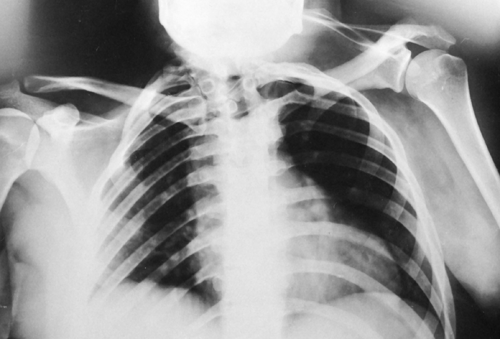 FIG. 8-16. Sprengel’s deformity. The left shoulder is affected. There is an associated abnormality of ossification of the cervical and upper thoracic vertebrae, with irregular segments fused together (Klippel-Feil deformity). These deformities frequently coexist. |
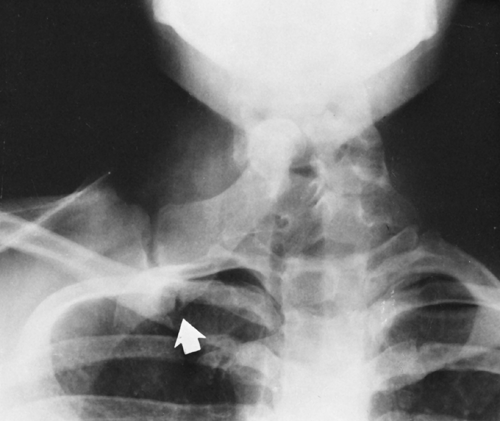 FIG. 8-17. The omovertebral bone in association with Sprengel’s deformity. The bone forms an articulation with the scapula (arrow) and the arch of one of the cervical vertebrae. |
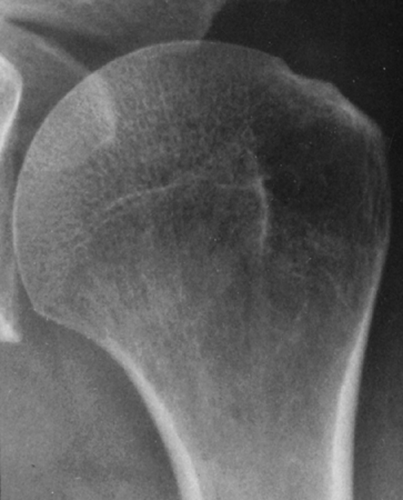 FIG. 8-18. Pseudocyst of the humeral head. A radiolucency is present within the greater tuberosity because of the relative absence of bone trabeculae. This is a frequent normal finding that is easily mistaken for evidence of metastatic disease or other abnormalities (see Fig. 8-34). |
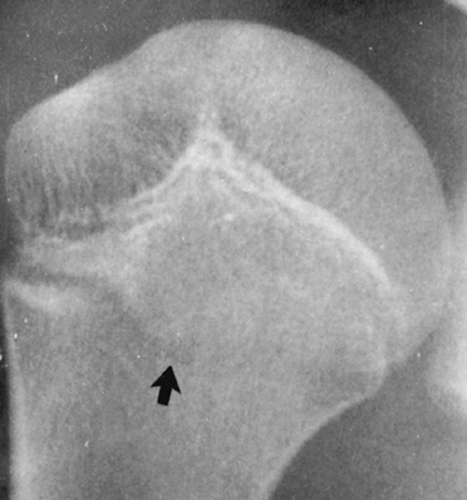 FIG. 8-19. Proximal humeral epiphysis. Anteriorly the growth plate is chevron shaped, whereas posteriorly it is transverse (arrow) and could be misconstrued as a fracture. |
 FIG. 8-20. Rhomboid fossa. The scalloped inferior margin of the medial clavicle (arrows) represents the site of insertion of the pectoralis muscles. It is present bilaterally in this case but may be seen unilaterally. |
 FIG. 8-21. Supraclavicular nerve foramen. The small lucency in the superior cortex of the middle third of the clavicle (arrow) represents a foramen for the supraclavicular nerve. |
 FIG. 8-22. Supracondylar process of the humerus. There is a hook-like projection of cortical bone arising from the medial surface of the distal shaft of the humerus. This is the characteristic location and position of the supracondylar process, which should not be mistaken for an exostosis. |
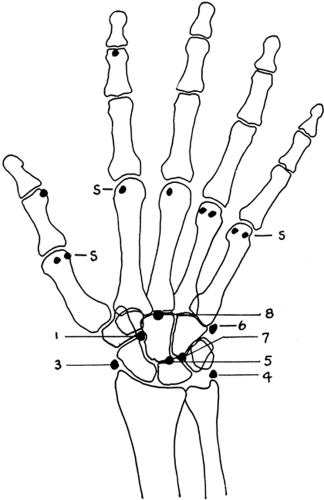 FIG. 8-23. The most frequent accessory ossicles in the hand and wrist. 1, os centrale; 3, os radiale externum; 4, os triangulate; 5, epilunatum; 6, os vesalianum manus; 7, epipyramis; 8, os styloideum; S, the most common sites for sesamoid bones in the hand. Number 2 is not included. |
 FIG. 8-24. Pseudoepiphyses and supernumerary epiphyses. The former are represented by incomplete clefts in the distal ends of proximal phalanges and proximal end of the fifth metacarpal. The latter are present at the proximal end of the second and fifth metacarpals and the distal end of the first metacarpal. |
 FIG. 8-25. Madelung’s deformity A: Oblique, B: Lateral, and C: PA projections demonstrate characteristic findings. The radius is curved and shortened in comparison to the ulna. The radial joint surface is tilted ulnarward and anteriorly. The hand is displaced anterior to the long axis of the forearm (B). The corpus assumes a triangular configuration (C). |
 FIG. 8-26. Carpal boss with os styloideum (arrow). A: Lateral view. B: Posteroanterior (PA) view. Bony prominence dorsally at the base of the second metacarpal as seen on the dorsum of the wrist (arrow) is not easily identified on the PA view. It is often difficult to determine on the plain films whether this is simply a bony protuberance or a separate ossicle, the os styloideum. |
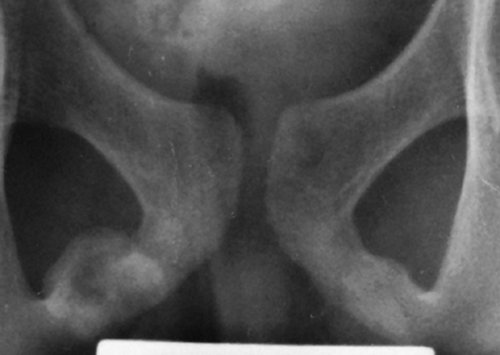 FIG. 8-27. Pubic synchondrosis in a 12-year-old. This represents the junction of the inferior ischial and pubic rami. The pattern of ossification is highly variable, often asymmetrical, and easily misinterpreted. |
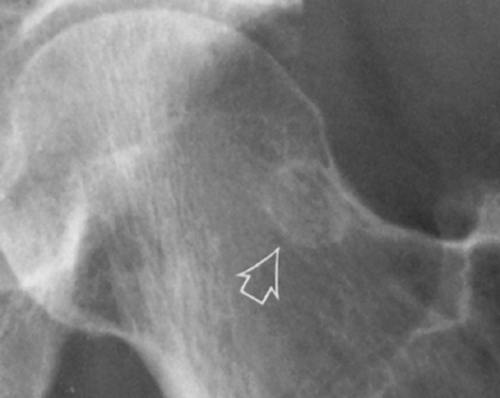 FIG. 8-28. Herniation pit of the femoral neck. Note the circular sclerotic radiodensity on the lateral margin of the femoral neck (arrow). In some cases, the pit may be smaller and the rim of sclerosis thicker. |
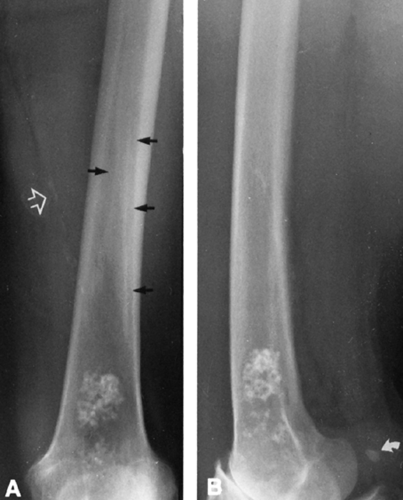 FIG. 8-29. Linea aspera—pilaster complex. A: The two long, roughly parallel lines (arrows) represent the margins of the pilaster complex on the posterior surface of the femur. This represents the site of insertion of the adductor muscles of the thigh. Calcification is present in the femoral artery (open arrow), and distally there is the conglomeration of calcium representing either an enchondroma or the residuals of previous bone infarct. B: Lateral view. Note the roughened surface of the posterior femoral cortex. This is the appearance of the pilaster complex or linea aspera when seen in profile. It is normal but could be misconstrued as evidence of periosteal new-bone formation. Note the fabella (arrow). |
 FIG. 8-30. Physiologic bowlegs. A: Initial views demonstrate moderate bowleg deformity. B: Approximately 1 year later, the bowing has largely disappeared. Note that the bowing involves both femur and tibia. |
 FIG. 8-31. Blount’s disease. There is bilateral involvement, with an angular deformity at the physis. The tibial shafts are straight and the femurs are uninvolved. |
 FIG. 8-32. Pellegrini-Stieda disease. A thin, shell-like calcification is seen at the superior margin of the medial femoral condyle (arrow). |
 FIG. 8-33. Cortical desmoid. Note the irregularity of the surface of the cortex of the distal femur (arrows) at the site of the insertion of the adductor magnus and gastrocnemius muscles. |
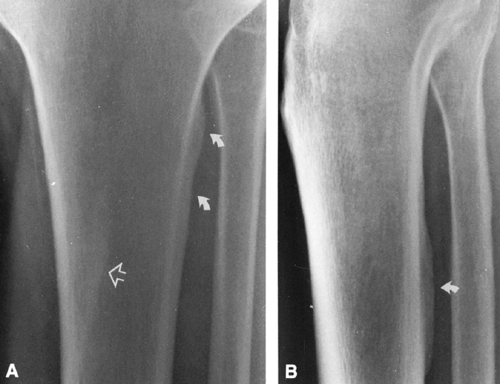 FIG. 8-34. Tibial tubercle and soleal line. A: Anteroposterior view. Prominent ossification of the interosseous membrane on the lateral surface of the tibia (arrows) is known as the tibial tubercle. This is commonly present but is of variable size. A similar ossification is present on the apposing margin of the fibula. The soleal line is seen on edge as an oblique line projecting in the medullary canal (open arrow). B: Lateral view. The soleal line is seen on the posterior surface of the tibial cortex (arrow). This may be misconstrued as evidence of periosteal new-bone formation associated with infection or stress fracture. The tibial tubercle cannot be seen on the lateral projection. |
 FIG. 8-35. Apophysis of the base of the fifth metatarsal. The secondary ossification center parallels the lateral aspect of the proximal end of the metatarsal. In this case, there is also an undisplaced transverse fracture (arrow) at the base of the fifth metacarpal. |
 FIG. 8-36. Bifid sesamoids. Both the medial and lateral sesamoids of the great toe are bifid (arrows). |
 FIG. 8-37. Pseudocyst of the calcaneus. The relative radiolucency beneath the tuber angle (arrow) represents an area devoid of trabeculae. This is a normal finding and is similar to the pseudocyst of the humeral head seen in Fig. 8-18. |
 FIG. 8-38. Congenital radioulnar synostosis with congenital dislocation of the head of the radius. There is bony fusion between the proximal radius and the ulna. |
 FIG. 8-39. Tarsal coalition, calcaneonavicular bar (arrow). Note also the thin, white line paralleling the distal tibial joint surface. This is an epiphyseal scar, the bony residua of the physis. |
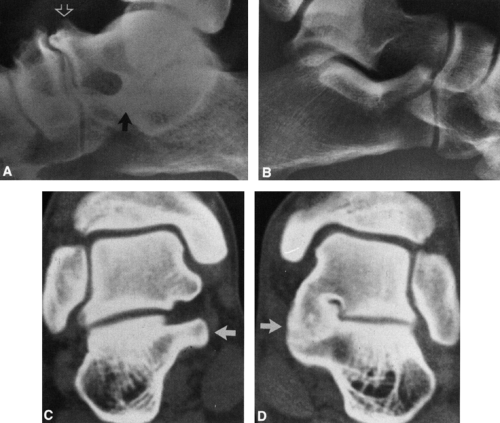 FIG. 8-40. Tarsal coalition, talocalcaneal fusion. A: Lateral view of the foot demonstrates pes planus, a prominent anterior beak of the talus (open arrow), and poor definition of the posterior facet of the talocalcaneal joint. There is a suggestion of fusion of the medial facet in the region of the sustentaculum tali (arrow). B: Normal side for comparison. C and D: Computed axial tomograms. Normal side (C) demonstrates normal appearance of sustentaculum tali (arrow). Affected side (D) demonstrates fusion of the medial facet of the talocalcaneal joint (arrow). |
The failure of segments to fuse is most commonly encountered in the spine, involving the laminae and spinous processes. This failure of fusion is known as spina bifida. When seen as an isolated radiographic abnormality, it is known as spina bifida occulta. It may be associated with other congenital abnormalities of the spine, as described in Chapter 12.
Bifid structures may also occur. These may develop from a natural growth, as in the bifid anterior margin of ribs (Fig. 8-4), or from a failure of fusion of structures that arise from more than one center, most commonly in the sesamoids of the great toe (see Fig. 8-36). Certain apophyses and epiphyses arise from multiple centers of ossification, which eventually fuse in most cases. Multiple centers of ossification are seen in the proximal humerus and elbow. The trochlear center of ossification of the elbow itself may arise from separate centers, as may the epiphyses of the proximal phalanx of the great toe. Less commonly, individual carpal or tarsal bones arise from separate centers of ossification.
Accessory centers of ossification and accessory bones are found rather frequently in the skeleton (Figs. 8-5 and 8-6). An accessory bone represents either a supernumerary ossicle not ordinarily found in the skeleton or a secondary center of
ossification that has failed to fuse and remains as a separate structure (Fig. 8-7). On occasion, they may predispose to injury or degenerative change and be responsible for symptoms.13, 15, 23 This is often associated with a positive bone scan in the region of the abnormality. Sesamoid bones (Fig. 8-8) arise in tendons, particularly those of the feet, and are very similar in appearance to accessory centers of ossification. These small accessory bones and sesamoids may be mistaken for pathologic conditions, particularly fractures, and knowledge of their distribution and frequency is therefore important.
ossification that has failed to fuse and remains as a separate structure (Fig. 8-7). On occasion, they may predispose to injury or degenerative change and be responsible for symptoms.13, 15, 23 This is often associated with a positive bone scan in the region of the abnormality. Sesamoid bones (Fig. 8-8) arise in tendons, particularly those of the feet, and are very similar in appearance to accessory centers of ossification. These small accessory bones and sesamoids may be mistaken for pathologic conditions, particularly fractures, and knowledge of their distribution and frequency is therefore important.
DIFFERENTIATION OF ANOMALOUS BONES FROM FRACTURES
A fracture line is ragged along its margin, irregular, and poorly defined; anomalous ossification centers and sesamoids are characterized by smooth cortical margins (see Figs. 8-5, 8-7, and 8-8). An avulsion or small fracture has an irregular, uncorticated surface at the line of fracture and a defect in the adjacent bone that corresponds to the avulsed fragment. Fresh fractures are accompanied by swelling of the contiguous soft tissue, which should not be present about an accessory center. Accessory centers and anomalous bones are commonly bilateral. Examination of the corresponding part of the opposite extremity is helpful in doubtful cases, but it is usually unnecessary. The precise diagnosis can usually be determined by reference to standard charts and diagrams (see Figs. 8-7 and 8-23).4
Normal Radiographic Findings Confused with Pathology
Nutrient Canals and Foramina
Nutrient canals are present in all the long and short tubular bones. These are fine, sharply marginated radiolucencies that extend obliquely
through the cortex, and they should not be mistaken for a fracture (Fig. 8-9). Nutrient canals are less radiolucent than a fracture and have a characteristic course. Nutrient foramina generally occur at the ends of bones, appearing as a small circular radiolucency, and are seen most commonly at the intercondylar notch of the knee.
through the cortex, and they should not be mistaken for a fracture (Fig. 8-9). Nutrient canals are less radiolucent than a fracture and have a characteristic course. Nutrient foramina generally occur at the ends of bones, appearing as a small circular radiolucency, and are seen most commonly at the intercondylar notch of the knee.
Interosseous Ridges
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


