LEARNING OBJECTIVES
1. Name and define the three zones of the airways.
2. Define a secondary pulmonary lobule and its appearance on high-resolution computed tomography (CT).
3. List the lobar and segmental bronchi of both lungs.
4. Identify the following structures on the posteroanterior chest radiograph:
• Lungs—right and left; right upper, middle, and lower lobes; left upper (including lingula) and lower lobes
• Pulmonary arteries—main, right, left, right interlobar, left lower lobe
• Airway—trachea, carina, main bronchi
• Fissures—minor, superior accessory, inferior accessory, azygos
• Aorta—ascending, arch (“knob”), descending
• Veins—superior vena cava, azygos, left superior intercostal (“aortic nipple”)
• Aortopulmonary window
• Right paratracheal stripe
• Junction lines—anterior, posterior
• Azygoesophageal recess
• Paraspinal lines
• Left subclavian artery
• Heart—right atrium, left atrial appendage, left ventricle, locations of the four cardiac valves
• Bones—spine, ribs, clavicles, scapulae, humeri
5. Identify the following structures on the lateral chest radiograph:
• Lungs—right and left; right upper, middle, and lower lobes; left upper (including lingula) and lower lobes
• Fissures—major, minor, superior accessory
• Aorta—ascending, arch, descending
• Retrosternal clear space
• Veins—inferior and superior vena cavae, left brachiocephalic (innominate), pulmonary vein confluence
• Brachiocephalic (innominate) artery
• Airway—trachea, upper lobe bronchi, posterior wall of bronchus intermedius
• Heart—right ventricle, right ventricular outflow tract, left atrium, left ventricle, locations of the four cardiac valves
• Pulmonary arteries—right, left
• Posterior tracheal stripe
• Hemidiaphragms—right, left
• Bones—spine, ribs, scapulae, humeri, sternum
6. Identify the following structures on chest CT:
• Lungs—right and left; right upper, middle, and lower lobes; left upper and lower lobes
• Fissures—major, minor, accessory (azygos, superior, and inferior)
• Pleura and extrapleural fat
• Airway—trachea, main bronchi, carina, lobar and segmental bronchi
• Heart—left ventricle, right ventricle, left atrium, right atrium, mitral valve, aortic valve, tricuspid valve, pulmonary valve, coronary arteries (left main, left anterior descending, left circumflex, right, posterior descending), coronary sinus
• Pericardium, including pericardial recesses
• Pulmonary arteries—main, right, left, right interlobar, segmental
• Aorta—ascending, arch, descending
• Arteries—brachiocephalic (innominate), common carotid, subclavian, axillary, vertebral, internal mammary, intercostal
• Veins—superior and inferior pulmonary, superior and inferior vena cavae, brachiocephalic, subclavian, axillary, internal jugular, external jugular, azygos, hemiazygos, left superior intercostal, internal mammary
• Bones—ribs, costochondral cartilages, clavicles, scapulae, sternum, spine
• Esophagus
• Thymus
• Thyroid gland
• Muscles—sternocleidomastoid, anterior and middle scalene, infrahyoid, pectoralis major and minor, deltoid, trapezius, infraspinatus, supraspinatus, subscapularis, latissimus dorsi, serratus anterior
• Aortopulmonary window
• Azygoesophageal recess
• Diaphragm
Anatomy is to physiology as geography is to history: it describes the theatre of events.
Jean Ferne (1497–1558), On the Natural Part of Medicine
A good radiologist knows the anatomy because knowing where structures normally “live” and recognizing the location of an abnormality helps to make or narrow the differential diagnosis. This chapter is an abbreviated review of thoracic anatomy as seen on chest radiographs and computed tomography (CT) of the chest. As a result of differences in patient age, body habitus, positioning, inspiratory effort, exam technique, and many other factors, normal anatomic structures will vary in appearance on chest radiographs from exam to exam, patient to patient, and even breath to breath. Some structures are not seen consistently (posterior junction line), whereas others are seen on most exams (left upper lobe bronchus on lateral view). Showing the myriad different appearances of normal anatomic structures is beyond the scope of this chapter; they are learned by paying close attention to and identifying normal structures on thousands of chest radiographs.
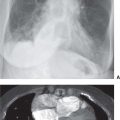
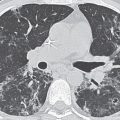
A frequent question of medical students and residents new to chest radiology is “How do you look at a chest radiograph?” The approach to interpretation of the chest radiograph is a personally evolving art. A person’s approach changes over time after seeing many chest radiographs. That answer doesn’t help the beginner, and so a few general “chest radiograph rules” are offered in Table 1.1, and reference standards are presented in Table 1.2. Normal anatomic structures are labeled on posteroanterior (PA) and lateral chest radiographs (Figs. 1.1 and 1.2) and axial CT images (Figs. 1.3 and 1.4). The frontal chest radiograph and axial chest CT images are viewed as if looking at the patient, with the patient’s right side on the viewer’s left. Lateral radiographs are, by convention, viewed with the patient facing to the viewer’s right (patient’s left side closest to the imaging plate).
ZONES OF THE AIRWAYS
The airways are composed of three zones. The conductive zone includes the trachea, bronchi, and nonalveolated bronchioles (air cannot diffuse through the well-developed wall). The transitory zone has both conductive and respiratory functions, and consists of respiratory bronchioles, alveolar ducts, and alveolar sacs. The respiratory zone consists of alveoli. The primary function of this zone is the exchange of gases between air and blood.
LUNG ARCHITECTURE
The primary pulmonary lobule consists of all alveolar ducts, alveolar sacs, and alveoli, together with their accompanying blood vessels, nerves, and connective tissues distal to the last respiratory bronchiole. This unit is too small to be seen radiologically. The secondary pulmonary lobule is the smallest discrete portion of the lung that is surrounded by connective tissue septae, and it is composed of three to five terminal bronchioles with their accompanying transitory airways and parenchyma (Fig. 1.5). A secondary pulmonary lobule contains 30 to 50 primary lobules, is polyhedral in shape and 1.0 to 2.5 cm in diameter, and can be appreciated on thin-section (1 to 2 mm) images of the lung. A pulmonary acinus is also an anatomic unit, defined as that portion of lung distal to the terminal bronchiole, comprising the respiratory bronchioles, alveolar ducts, alveolar sacs, and alveoli. Typically, 6 to 12 acini are grouped together in a secondary pulmonary lobule (1).
Table 1.1 INTERPRETATION OF THE CHEST RADIOGRAPH: “RULES” TO FOLLOW
1. When you have them, always look at both views (PA and lateral). To confirm that pathology is within the chest, it must usually be seen in the chest on both views.
2. The right heart border is formed by the right atrium, and it is obscured by medial segment right middle lobe processes (disease limited to the lateral segment will not obscure the right heart border).
3. The left heart border is formed mainly by the left ventricle and is obscured by lingular processes.
4. The right diaphragm is usually 1.5 to 2.0 cm higher than the left.
5. The diaphragm is obscured by lower lobe processes (unless only the superior segment of the lower lobe is involved).
6. Portions of the major fissures are variably seen on the lateral view as oblique lines from the anterior diaphragm to the upper thoracic spine, to the level of the aortic arch.
7. The minor fissure is on the right, separating the right upper lobe from the right middle lobe. It courses from the right hilum to the right lateral anterior chest wall and is variably seen on PA and lateral chest radiographs.
8. Normal hilar opacities are predominantly caused by the pulmonary arteries and should be symmetric in size and density.
9. The aortic arch, or “knob,” is above the left hilum. (Watch out for the right aortic arch variant!)
10. The trachea is midline but may be deviated to the right or forward from a tortuous aorta.
11. The costophrenic angles should be sharp on both views (sharp enough to pick your teeth with), except in patients with severe pulmonary emphysema, resulting in flattening of the hemidiaphragms.
12. With good inspiratory effort, the size of the heart on the PA radiograph is normally ≤50% of the widest diameter of the thoracic cage.
13. Right middle lobe and lingular processes are projected over the heart on the lateral view.
14. A young healthy person can take a breath deep enough to inflate the lungs to the level of the 10th rib posteriorly (or the 6th rib anteriorly).
15. Opacity of the lungs should be symmetric unless the patient is rotated.
16. The stomach bubble is under the left hemidiaphragm. (Watch out for situs inversus.)
17. Don’t forget to look at the bones and soft tissues.
Table 1.2 SIZE AND DENSITY RATIOS ON THE PA CHEST RADIOGRAPH
Size
Cardiothoracic The heart diameter should be half or less than half of the chest diameter. An easy way to eyeball this—assuming the spine is straight and in the middle of the chest—is to see if the heart to the right of the midline fits between the left heart border and the left ribs.
Aortopulmonary The left pulmonary artery, as it passes over the left main bronchus, should be less than the width of the aortic knob. The aortic arch is approximately 3 cm above the carina in adults until the aorta begins to get tortuous. The left pulmonary artery is approximately 3 cm down the left main bronchus and then ascends up and out at approximately
45 degrees.
Azygotracheal The azygos vein, if visualized (at the right tracheobronchial angle), should be no wider than approximately one-half the width of the trachea, and its height should be no greater than the width of the trachea.
Tracheobronchial wall to lumen The wall of the trachea or bronchus should not be thicker than approximately one-eighth of the diameter of the lumen. The tracheal diameter should be equal on the PA and lateral views and should be less than the width of a vertebral body.
Right lower lobe artery to trachea The right lower lobe pulmonary artery should not be wider than the width of the tracheal lumen.
Hilar height The left hilus should be approximately 2 cm higher than the right, because the left pulmonary artery has to go over the left main bronchus.
Arteriobronchial An artery and its accompanying bronchus should be the same size (seen best “end-on”).
Density
Cardiohepatic The heart should be about half as dense as the middle of the liver (it’s about half as thick). This reference requires good exposure. Beware the “ivory heart” of left lower lobe collapse.
Intracardiac The heart should be the same density on each side of the spine.
Intrahepatic The top of the liver should be about half as dense as the middle, because it’s about half as thick, provided the diaphragm domes normally.
Right paratracheal–aortic The density to the right of the trachea at the level of the aortic arch should never be as great or greater than the density of the aortic knob.
Hilar The hila should be the same density (they are composed of the same vascularity).
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


