• Radiography, bone CT most useful for bone anatomy
Top Differential Diagnoses
• Traumatic or degenerative vertebral subluxation
• Transverse process fracture
• Vertebral segmentation and formation anomalies
• Vertebral hemangioma
• Intervertebral disc herniation
• Nerve sheath tumor
• Posterior spinal dysraphism
• Caudal regression spectrum
Clinical Issues
• Discovered incidentally when patient is imaged for other indications
Patient asymptomatic, or presenting symptoms do not match location of finding
• Normal life expectancy, no incremental morbidity
• May lead to unnecessary diagnostic tests or treatment if not recognized as normal variant
Diagnostic Checklist
• Many normal variants are common and readily recognized by experienced observers
• Some are uncommon and may not be recognized as normal variant, require high index of suspicion to correctly diagnose
• Consider normal variant within differential diagnostic considerations when unexpected finding is detected
(Left) Sagittal bone CT in a young pediatric patient demonstrates slight apparent subluxation of C2 on C3 . All other spinal lines are normal, particularly the posterior spinolaminar line from C1 to C3, confirming pseudosubluxation.
(Right) Anteroposterior cervical radiograph shows unusual elongation of the C7 transverse processes . In some patients, draping of the lower brachial plexus trunk over the C7 transverse process may produce a clinical brachial plexopathy.
(Left) Anteroposterior cervical radiograph demonstrates small bilateral rudimentary C7 cervical ribs . Downward angulation of the adjacent transverse processes distinguishes these from hypoplastic T1 thoracic ribs.
(Right) Sagittal T1WI MR along the plane of the medial aspect of the L5 pedicle shows a vertically oriented root spanning the L5 disc level due to a conjoined nerve root. This vertical orientation of the exiting inferior root is typical, along with the more horizontal course of the superior root.
TERMINOLOGY
Definitions
• Normal anatomical variations that simulate pathological conditions
IMAGING
Cervical Vertebral Pseudosubluxation
• Classically most conspicuous at C2/3 level, with apparent anterior subluxation of C2 on C3 with head in flexed position
• Observed in younger pediatric patients with incomplete ossification of upper cervical spine
Prevalence in older patients controversial, may represent true ligamentous injury
• Absence of spinolaminar line disruption and patient age keys to correct recognition
Incomplete C1 Ring
• C1 ring is incompletely ossified
• In absence of neurological abnormalities or documented instability, asymptomatic normal variant detected during imaging for other reasons
Cervical Ribs
• Small rudimentary ribs at C7
Elongation of C7 transverse processes is close variant with similar clinical findings
• Usually asymptomatic but may produce brachial plexopathy or thoracic outlet symptoms
• Orientation of transverse processes key to distinguishing cervical from thoracic ribs
Cervical transverse processes point caudal, while thoracic transverse processes point rostral
Transitional Vertebral Anatomy
• Variant osseous anatomy at thoracolumbar or lumbosacral transitions
• Common variants include S1 “lumbarization,” L5 “sacralization,” rudimentary L1 ribs, hypoplastic T12 ribs
• Confound correct counting of vertebral levels
Usually not clinically significant issue if counting method well described in imaging report
• May predispose to accelerated degenerative changes at mobile segments above or below variant levels
Focal Fatty Marrow
• Focal fat conglomeration within vertebral marrow
• Follows fat signal and density on all sequences
Fat-saturation MR sequences helpful to confirm diagnosis
• Primary clinical impact is mimicry of vertebral hemangioma
Ectopic Kidney
• Pelvic kidney lower than orthotopic location, more midline than expected
Only gold members can continue reading. Log In or Register to continue










 . All other spinal lines are normal, particularly the posterior spinolaminar line
. All other spinal lines are normal, particularly the posterior spinolaminar line  from C1 to C3, confirming pseudosubluxation.
from C1 to C3, confirming pseudosubluxation.
 . In some patients, draping of the lower brachial plexus trunk over the C7 transverse process may produce a clinical brachial plexopathy.
. In some patients, draping of the lower brachial plexus trunk over the C7 transverse process may produce a clinical brachial plexopathy.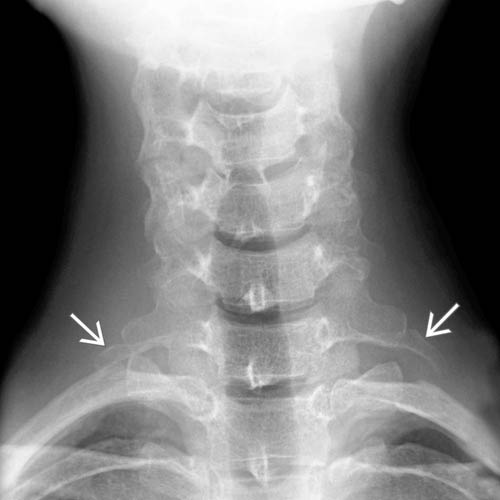
 . Downward angulation of the adjacent transverse processes distinguishes these from hypoplastic T1 thoracic ribs.
. Downward angulation of the adjacent transverse processes distinguishes these from hypoplastic T1 thoracic ribs.
 spanning the L5 disc level due to a conjoined nerve root. This vertical orientation of the exiting inferior root is typical, along with the more horizontal course of the superior root.
spanning the L5 disc level due to a conjoined nerve root. This vertical orientation of the exiting inferior root is typical, along with the more horizontal course of the superior root.









