Fig. 36.1
This patient complained of rotational instability of his ankle joint after recurrent ankle sprains in sports. SPECT/CT and MRI both showed a large OCL of the medial talar shoulder. However, SPECT/CT depicted the extent of subchondral cyst formation more clearly and localised the metabolic active region to a much smaller area compared to the area of oedema in the MRI. SPECT/CT is used to decide to what extent the subchondral bone needs to be reconstructed
Fig. 36.2
This 40-year-old active snowboarder sustained a fall and ankle sprain in his snowboarding boots one year ago. Because of persistent pain, MRI and SPECT/CT were performed. Both revealed an osteochondral lesion in the centrolateral joint compartment. This example illustrates how much more precise bony structure can be analysed on SPECT/CT images when compared to MRI. Moreover, in SPECT/CT, there is increased tracer uptake at the talar and the tibial side. This information guides further treatment as both lesions have to be addressed
36.2.2 Stress Fracture s
Stress reactions and fractures around the ankle, especially in the distal tibia and fibula, are important overuse injuries in endurance athletes. While bone scan (Spyridonidis et al. 2014; Krestan et al. 2011) and MRI are established diagnostic tools (Sijbrandij et al. 2002), the sensitivity and specificity for SPECT/CT will have to be determined first. However, a more prominent role of SPECT/CT in the future is likely, since this modality combines the advantages of bone scintigraphy which shows metabolic activity, and CT may show osteopenia, the earliest finding in early stress fracture (Gaeta et al. 2005; Mohan et al. 2010) (Fig. 36.3).
Fig. 36.3
This 62-year-old patient with known posttraumatic upper and lower ankle osteoarthritis presented with right-sided ankle pain. SPECT/CT indicated a stress fracture of the anterior tibia due to the deformity caused by the previous trauma
36.2.3 Ankle Impingement
Ankle impingement can be due to abnormal configuration of articulating bones; extreme movements of normally shaped joint partners, e.g. in ballet dancers; accessory bones interfering with otherwise normal joint partners, e.g. os trigonum or as a result of osteophyte formation around the ankle due to degenerative processes, e.g. in soccer’s ankle. It can be located anteriorly (e.g. soccer’s ankle) or posteriorly (e.g. dancer’s ankle). Only in true osseous impingement, bone scan and SPECT/CT play a role, since soft tissue impingement cannot be depicted with current nuclear imaging methods. However, most cases of bony impingement (in particularly anterior impingement) can sufficiently be diagnosed using conventional X-rays or MRI. SPECT/CT might help in unclear cases of persistent ankle pain and then identifies, e.g. an impinging os trigonum with increased metabolic uptake as a reason for deep or posterior ankle pain. In these patients, SPECT/CT is a richer source of information (Fig. 36.4).
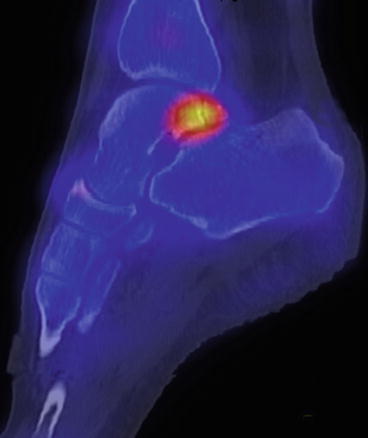
Fig. 36.4
This 27-year-old female patient presented with diffuse ankle pain while running and signs of posterior impingement in maximal plantar flexion. Conventional X-rays showed a mostly normal ankle except for an os trigonum (DD chronic fracture of the posterior talar process). SPECT/CT shows the metabolic activity of the os trigonum which correlated with pain origin. The patient was pain-free after excision of this accessory bone
36.2.4 Fracture s and Nonunion s
Nuclear medicine techniques have no role in diagnosing acute traumatic fractures. However, SPECT/CT might help finding a) stress fractures (see above) or b) persistent pain in the context of an already detected and treated fracture. It is able to precisely show osseous nonunion as well as associated metabolic uptake representing symptomatic pseudoarthrosis (Figs. 36.5 and 36.6).
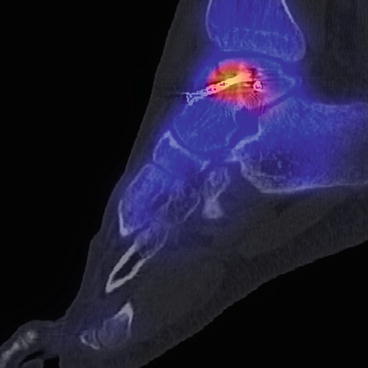
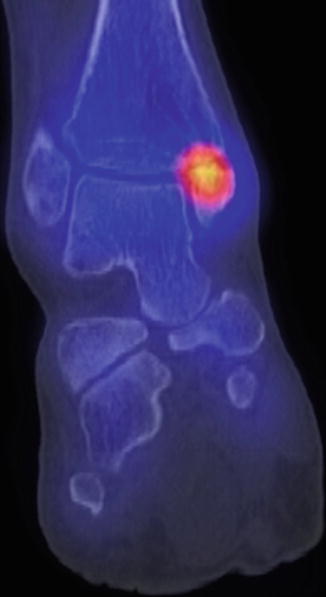
Fig. 36.5
This patient suffered a multifragmentary talar body fracture. Persistent pain nine months post-surgery led to further imaging studies. SPECT/CT clearly showed a nonunion of the anterior fracture region and increased metabolic uptake at that same region which make it likely the origin of the pain in this patient
Fig. 36.6
This 30-year-old patient sustained a Maisonneuve-type fracture including a proximal fibular fracture and a displaced medial malleolar fracture. Nine months after open reduction and internal fixation at the medial malleolus, an atrophic nonunion was identified showing absent bridging callus and increased tracer uptake as signs of nonunion
36.2.5 Bone Bruise s and Osteonecrosis
It is very interesting to see the differences of the size of the bone bruise/bone oedema in the MRI and the focal activity in the SPECT/CT. This is not only true for osteochondral lesions like discussed above but also for perfusion-based disorders such as avascular talar necrosis or chronic regional pain syndrome. While SPECT/CT specifically highlights metabolic activity of osteoblasts, for oedema pattern in MRI, it has been shown that this histologically equals a number of noncharacteristic histological abnormalities which make interpretation difficult (Zanetti et al. 2000). For atraumatic medial knee pain, it has even been shown that scintigraphy is more sensitive than MRI (Buck et al. 2009) (Fig. 36.7).
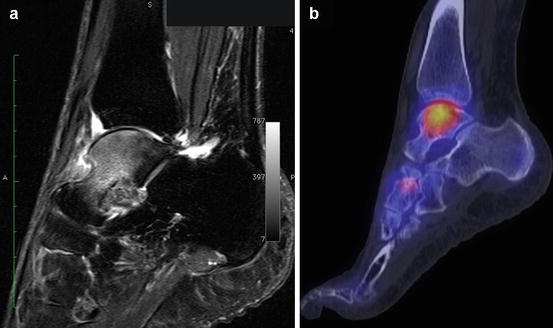
Fig. 36.7




Unexplained ankle pain in a 70-year-old lady, who used to hike several hours a day. MRI (a) showed signs of a – idiopathic – talar necrosis. This was confirmed in SPECT/CT. However, this example shows very well, that the lesion size on MRI (representing bone oedema, a) is much larger, than on SPECT/CT (representing tracer uptake and remodelling of the bone, b). It can also be located to a particular part of the talar body rather than the whole talus. Thus, SPECT/CT helped to determine the region of bone to be treated and to exclude early ankle osteoarthritis. Therefore, a well-directed, arthroscopically guided retrograde drilling through the sinus tarsi could be chosen as minimal invasive therapy
Related posts:



Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
