Fig. 21.1
Normal aspect of the elbows on a three-phase bone scintigraphy using 99mTc-HDP (injection site of the foot). Normal flow (a) and blood pool phase (b). Normal distribution of bone tracer in the osseous structures of the elbow joint (late images, c posterior view, d lateral view)
Only in very specific diagnoses, including (stress) fractures, lateral and medial epicondylitis, osteochondritis dissecans, and (a)septic loosening of prosthetic implants, nuclear medicine is able to play an additional role in imaging the elbow. A three-phase bone scintigraphy, using a technetium-99m (99mTc)-labeled diphosphonate complex, is the cornerstone within nuclear medicine imaging and can detect fractures, prosthesis loosening, and inflammation. The exact role of bone scintigraphy in loosening of elbow prostheses is still a matter of debate. Uptake around the prosthesis can be physiological due to “recent” surgery, up to 2 years after implantation, in accordance with total knee arthroplasty. An additional leukocyte scintigraphy, usually with 99mTc-labeled hexamethylpropyleneamine oxime (99mTc-HMPAO), is able to distinguish between no infection, inflammation, or infection (Fig. 21.2). A negative leukocyte scan excludes an infection. This chapter highlights the role of nuclear medicine in injuries of the elbow and the forearm.
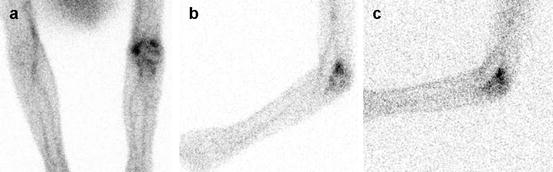
Fig. 21.2
Leukocyte scintigraphy, using 99mTc-HMPAO-labeled autologous white blood cells, in a patient after a distal humeral fracture on the right side with complaints of functional restrictions. Early (after 3 h) images of the elbow region, posterior view (a) and lateral view (b), showing abnormal uptake in the proximal part of the right elbow. Late image (c, after 24 h), lateral view showing persisting increased uptake at the right elbow. The ratio of abnormal uptake to the contralateral normal side increases, indicating an active infection, in this case, osteomyelitis
21.2 Lateral and Medial Epicondylalgia
As described in Chap. 19, lateral epicondylitis, also known as lateral epicondylalgia or “tennis elbow,” is defined as an overuse injury of the common extensor tendon, which originates from the lateral epicondyle of the humerus. Medial epicondylitis, also known as medial epicondylalgia or golfer’s elbow, concerns a (degenerative) tendinopathy of the common tendinous origins of the flexor muscles of the fingers, thumb, and wrist, which is inserted into the medial epicondyle of the humerus (Rineer and Ruch 2009). Also, this epicondylalgia is described in detail in Chap. 19.
These both indications are the most common reasons for making a three-phase bone scintigraphy of the elbow joint. However, only few data are available in literature. In fact, only one large study is published that reported the use of three-phase bone scintigraphy in patients with chronic epicondylalgia, with poor response to or failure of traditional conservative treatment (Pienimäki et al. 2008). In this study, 59 patients with unilateral chronic epicondylalgia underwent history and pain questionnaires, physical examination including manual testing, and bone scintigraphy using 550 MBq 99mTc-labeled hydroxy methane diphosphonate (99mTc-HDP). A semiquantitative method was used to determine the ratio between the uptake in the affected epicondyle and the ipsilateral humerus, as well as in the unaffected healthy epicondyle and the humerus.
Flow (perfusion) and blood pool images, available in 52 and 54 patients, respectively, were abnormal in 7 (13 %) and 12 (22 %) patients and indicate increased soft tissue uptake suggested to be a consequence of vasodilatation due to chronic prolonged inflammation. Tracer uptake on late static images was categorized as low, slightly elevated, moderately elevated (15 patients in all three categories), and high (14 patients). At the affected epicondyles, tracer uptake was significantly higher compared to the corresponding healthy epicondyle: epicondyle-to-humerus ratio was 33 % (p < 0.001) higher in men and 17 % (p = 0.007) in women. However, in men, the uptake in the affected epicondyle was higher than in women. High bone tracer uptake was present in 14 patients and was associated with significantly better reported work ability, better function of the arm, and less muscle tenderness. Therefore, the authors concluded that high tracer uptake might reflect a regenerative healing process of epicondylitis. Furthermore, they concluded that bone uptake might enable subclassification of patients with epicondylitis, which could be of value in designing treatment interventions for this highly prevalent disorder.
In general daily practice, three-phase bone scintigraphy in epicondylalgia is mainly used to confirm or exclude this diagnosis when the referring clinician is in doubt about the diagnosis. Three phase bone scan may help in localizing the site and severity. Depending on severity of inflammatory response, increased uptake may be seen both on early and late phases (Patel 1998). A statement on prognosis is regularly not reported.
21.3 Other Elbow and Forearm Injuries
Other elbow and forearm injuries are mentioned only in case reports or small case series and sometimes even not. The following contains an overview of the role of nuclear medicine in these different diagnoses.
Olecranon bursitis may show positive flow and blood pool images on the bone scan due to inflammation of the bursa but is not supposed to give positive results on the late images, since those images only reflect bone metabolism. On FDG-PET, however, it is sometimes seen as an occasional finding in patients. Uptake of FDG around the elbow joint may indicate that the patient suffers from bursitis.
One report describes the use of three-phase bone scintigraphy in diagnosing triceps tendinopathy in amateur weight lifters (Van der Wall et al. 1999b). Twelve patients with different upper arm complaints after weight lifting underwent three-phase bone scintigraphy using 850–900 MBq 99mTc-MDP. Two patients were reported to have triceps tendinopathy, one patient bilaterally. In both patients, it was different from the clinical diagnosis, by history and physical examination. One patient, a male runner, was clinically diagnosed with tendinopathy of the supraspinatus muscle; the other patient, a female tennis player, was suspected of having synovitis of the elbow. This report showed that nuclear medicine is able to play a diagnostic role in confirming clinically suspected injuries of the elbow and, additionally, detect unsuspected disease.
Posterior impingement is an uncommon disorder in the general population, however, not in athletes with repetitive stretching of the elbow. CT can be used to evaluate the posterior compartment for osteophytes. MRI with intra-articular contrast is even more sensitive, with sensitivity reported for posterior soft tissue or loose bodies nearly 90 % (Eygendaal and Safran 2006). Bone scintigraphy – with SPECT-CT – will also be able to visualize these osteophytes and may be helpful to determine viability of the loose fragment. This technique was found useful for localizing and characterizing impingement syndrome and soft tissue pathology in the ankle and foot region (Chicklore et al. 2012). Literature studies that describe the use of nuclear medicine imaging techniques in posterior impingement of the elbow are not available.
Osteochondritis dissecans (OD) typically affects the humeral capitellum of the dominant elbow in athletes engaged in repetitive overhead or upper extremity weight-bearing activities. As mentioned before, MRI is the gold-standard imaging technique since it shows osteochondral lesions of the capitellum at an earlier stage, is more accurate in showing the presence of loose bodies, and appears to be more valuable in determining the stability and viability of the OD fragment (Van der Ende et al. 2011). Reports mentioning the use of bone scintigraphy for OD are scarce and mostly older publications (Hall and Galea 1999; Van der Wall et al. 1999a; Woodward and Bianco 1975). However, bone scintigraphy could be of use for this indication, since it may show positive results in all three phases. SPECT imaging and correlation with CT may show high accuracy for viability of loose fragments.
Stress injuries to the medial elbow are well documented. Magnetic resonance imaging is the modality of choice. The role of nuclear medicine, especially bone scintigraphy, is limited to the situation in which conventional imaging is not able to identify a lesion. However, bone scintigraphy can be of value since injured or degenerative medial collateral ligaments may show calcifications (Mirowitz and London 1992). A stress lesion to the proximal medial ulna, in the region of the medial collateral ligament, seen on a three-phase bone scan was reported once (Mamanee et al. 2000). This 14-year-old baseball player (pitcher) suffered from increasing pain in his right medial elbow since three months. After a short period of rest, the complaints disappeared, and he was able to pitch with no symptoms.
Stress fractures in throwers are generally located proximal to the elbow, whereas weight lifters usually suffer from stress fractures distal to the elbow. Bone scintigraphy is able to visualize fractures in these patients when conventional imaging is indecisive (Sinha et al. 1999).
Little leaguer’s elbow is described as an apophysitis of the medial epicondyle in young athletes, due to repetitive valgus stress of the elbow (Cassas and Cassettari-Wayhs 2006; Shanley and Thigpen 2013). The diagnosis is made primarily clinically and should be considered in throwers with medial elbow pain. Plain radiograph imaging will suffice, however, may also be normal. MRI provides additional detail and is considered to be a helpful tool as well (Benjamin and Briner 2005). So far, no reports of nuclear medicine modalities are available for this specific indication.
Nuclear medicine modalities are regularly not performed in patients suspected of an acute and chronic forearm compartment syndrome. No reports are available which discuss the diagnostic value for these indications. One case report mentions uptake of 99mTc-labeled methylene diphosphonate (MDP) in the forearm due to an acute compartment syndrome (Gerard et al. 2008). Initially, the bone scan in this patient was performed to detect osseous metastases in a patient with bladder cancer. The compartment syndrome was caused by infiltration of high-volume intravenous contrast, administered during a CT scan the day before.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


