Acute injury
Overuse injury
Muscle contusion
Fatigue fracture
Ligament sprain
Spondylosis
Joint sprain
Spondylolisthesis
Traditionally, three-phase bone scintigraphy is commonly exploited in the evaluation of athletes with traumatic pain. The high-contrast resolution of bone scan allows early detection of acute spine trauma when imaging is performed within 6–72 h following the onset of symptoms.
SPECT/CT in particular can complement the management of sports-related stress injuries when structural imaging methods, i.e. radiography or computed tomography failed to yield adequate information on their sites and nature of the attributed abnormalities.
Bone stress injuries account for about 10 % of general sports medicine practice (Anshu 2010; Traughber and Havlina 1991). Lower extremity bones are most commonly affected (70–95 %) followed by the spine.
Bone scintigraphy with SPECT/CT has high diagnostic accuracy in localising acute stress reactions and stress fractures involving the posterior elements of the spine (Fig. 12.1). SPECT/CT images confirm a fracture by high metabolic activity at the site of injury and the absence of osteoblastic or osteolytic pathology connote active degenerative osteoarthrosis.
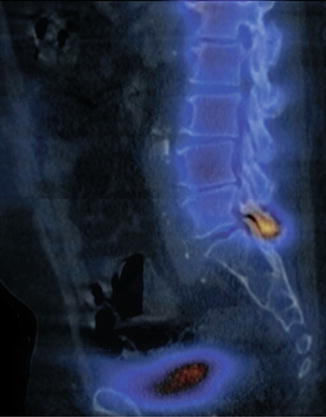
Fig. 12.1
L5 pars fracture. A 66-year-old female with lower back pain. MIP 99mTc-MDP SPECT/CT image shows the location of the metabolic activity indicating an acute stress reaction of the pars interarticularis without an obvious fracture
Stress fractures will show a focal abnormal uptake corresponding to the fracture defect seen on the computed tomography (CT) of the fused SPECT/CT. Focal uptake in the pars or pedicle of the lumbar spine, without any morphological abnormality, is consistent with a stress reaction (pre-fracture phase) and ascertains the reason for back pain in an athlete (Anshu 2010).
12.3 Overuse-Related Injuries
Overuse injuries of the spine are more subtle and usually occur over time in a repetitive manner as a result of micro-trauma to the tendons, bones, and joints. “High-risk” overuse injuries render a long period of recovery with significant loss of time from sports participation. These include certain stress fractures, physeal stress injuries, spondylosis, spondylolisthesis, and sacroiliac joint injury/inflammation (Table 12.1).
12.3.1 Fatigue Fracture
Fatigue fractures are also related to the chronic repetitive stress applied to healthy bone (Southam et al. 2010). An example of this is the fatigue fracture of the sacral spine (Fig. 12.2). A vertical concentration of cycling overloading in the sacral bone combined with impaired shock absorption due to associated muscle fatigue has been postulated as a potential mechanism in regard to sacral fatigue fracture pathogenesis (McFarland et al. 1996). High-intensity training or rapid changes in training system are common predisposing factors (Major et al. 2000). Leg length discrepancy, footwear more than 6 months old, poor training surface, nutritional deficiencies, and the female athlete triad have also been implicated as risk factors, among others (Major et al. 2000; McFarland et al. 1996).
Fig. 12.2
A 62-year-old female with a fatigue fracture of the ala sacrum. Coronal 99mTc-MDP SPECT/CT image reveals an “H”-shape configuration sign
This type of fracture causes often an unsuspected and undiagnosed local limb pain in athletes. To ensure early diagnosis when an effective selective treatment is required, bone scintigraphy with SPECT/CT will be a useful tool especially in recognising high bone turnover as signalled by increased MDP metabolic activity.
12.3.2 Spondylosis
Spondylosis is an age-related chronic process defined as the development of vertebral osteophytes, succeeded by osteochondrosis related to disc disease with disc space narrowing and secondary osteoarthritis of the facet joints. Premature spondylotic changes are likely to affect athletes with a history of vigorous load-bearing body stress activities. The more advanced stages of the process may produce a wide range of symptoms related to neuronal conflict of osteophytes or disc protrusion and facet osteoarthritis including pain. The degenerative disc changes include desiccation of the nucleus pulposus, loss of annulus fibrosus elasticity, and narrowing of the disc space with or without disc bulging or protrusion with or without annulus fibrosus rupture. Spondylosis is most often non-symptomatic. Not infrequently, however, these patients will have very few neck symptoms and will present with referred pain patterns: occipital headaches and pain in the shoulder, suboccipital and intrascapular areas, and anterior chest wall.
In certain circumstances, bone scintigraphy with SPECT/CT may have a complementary role to plain radiography and CT in isolating the site of increased bone turnover as signalled by marked uptake of MDP (Fig. 12.3). Spondylolysis has been reported to be the most common cause of lower back pain seen in a sports medicine clinic (Stasinopoulos 2004). It remains the major cause of spondylolisthesis and spine instability. AP and standing lateral lumbar radiographs are supplemented by oblique views. On oblique views the defect is seen as the so-called fracture in the “neck of the Scotty dog”. Collier et al. and others reported that SPECT is more sensitive than planar bone scintigraphy in the identification of symptomatic sites in spondylolysis (Collier et al. 1985). SPECT improves the detection of spondylolysis compared to planar bone scintigraphy (Bellah et al. 1991).
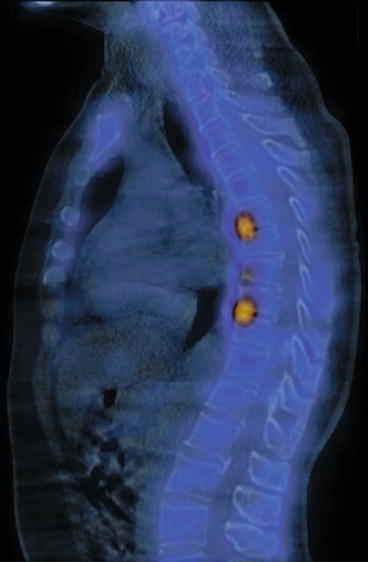
Fig. 12.3
A 29-year-old female with back pain. MIP 99mTc-MDP SPECT/CT shows increased metabolic activity in the disc plates of the lower thoracic spine with T9 and C10 anterior wedging denoting chronic spondylosis
For spondylolysis or stress fracture in athletes, bone scintigraphy with SPECT/CT was found more sensitive than lumbar MRI; this is related to the non-visualisation of the pars interarticularis on MRI examinations performed for disc disease (Masci et al. 2006). A SPECT/CT bone scan is also recommended for those cases in which a pars defect is suspected on plain radiographs. It may help to determine if a pars defect seen on X-ray is “hot” and therefore likely to be a cause for the pain. Most frequently, spondylolysis is associated with repetitive microtrauma, occurring in the adolescent during spinal growth. An increased incidence of spondylolysis is seen in adolescent athletes who practice sports with repetitive and excessive hyperextension such as gymnastics, diving, ballet, and soccer (d’Hemecourt et al. 2000, 2002).
12.3.3 Spondylolisthesis
Spondylolisthesis is a spinal condition in which all or a part of a vertebra has slipped forward on another (Fig. 12.4). There are several types of spondylolisthesis, but the most common in sports are stress fractures in the isthmus or pars interarticularis (Seimon 1983). The most common clinical manifestation of spondylolisthesis is lower back pain. Although the cause of this type of back pain in the adult has been studied extensively, its origin is still unclear. Bone scintigraphy with SPECT/CT has a role when the acuity of a pars defect is in question and it can be documented within 3 months after the injury; if the defect is longer existing, the scan will become negative.
Fig. 12.4
A 46-year-old male with L4–L5 pars interarticularis defect. MIP 99mTc-MDP SPECT/CT shows increased metabolic activity at the site of a L4–L5 interarticularis fracture resulting in anterolisthesis of L3 on L4 vertebra. The axial CT image confirms presence of the fracture involving the right pars interarticularis (arrowed)
12.4 Specific Spine Injuries
12.4.1 Acute and Chronic Lumbago
Pain in the lower back in athletes can be caused by a variety of conditions including musculo-ligamentous, osteoarticular, and neurologic disorders. It is a common source of pain in athletes, leading to significant time missed and disability (Petering Ryan and Charles 2011). Undifferentiated lower back pain in the general population is a well-established indication for planar bone scintigraphy (Bombardieri et al. 2006; Kanmaz et al. 1998). SPECT/CT imaging is useful for anatomic and functional evaluation of benign and malignant spine bone diseases, particularly for evaluation of chronic back pain (Schillaci 2005). Mechanical lower back pain accounts for up to 97 % of lower back pain diagnoses in the general population (Kalichman and Hunter 2007; Deyo and Weinstein 2001). A clinical examination of mechanical lower back pain is non-specific and is not able to discriminate vascular, infectious, inflammatory, and neoplastic aetiologies. Lumbar facet joint capsules are richly innervated with autonomic nerve fibres and may become a potential source of pain (Willard 1997). Lower back pain getting worse when sitting may indicate a herniated lumbar disc. Pain with acute onset may suggest a herniated disc or a muscle strain, as opposed to a more gradual onset of pain, which fits more with osteoarthritis, spinal stenosis, or spondylolisthesis (Table 12.2).
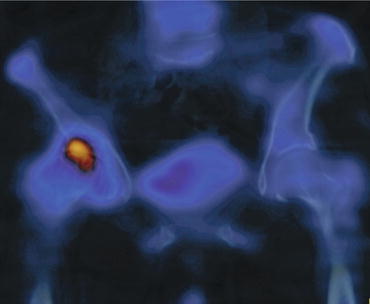
Table 12.2
Pain and the potential attributes
Symptoms | Causes |
|---|---|
Acute and chronic local pain | Direct trauma, spondylolisthesis, sacral insufficiency fracture, facet joint osteoarthritis |
Sciatica | Disc prolapse |
Referred pain (Fig. 12.5) | Osteoarthritis of knee or hip joint |
Fig. 12.5
A 44-year-old female with right lower lumbar pain. MIP 99mTc-MDP SPECT/CT shows increased metabolic uptake of the right hip joint representing osteoarthritis as a cause of referred pain to the lower lumbar region
Sports persons who continue to complain of lower back pain for more than 6 weeks should have plain radiographs including oblique views (Logroscino et al. 2001). The vast majority of patients with predominantly lower back pain will have normal plain radiographs. In these patients with suspected clinically bone abnormality, bone scintigraphy with SPECT/CT may be considered as a second-line imaging test (Table 12.3).
Table 12.3
Differential diagnosis of lower back pain and diagnostic imaging tools that may be indicated
Evaluation | Back sprain | Disc prolapse | Spinal stenosis | Spondylolisthesis | Spondyloarthropathy | Infection | Tumour | Metabolic |
|---|---|---|---|---|---|---|---|---|
Predominant pain | Back | Leg | Back/leg | Back | Back | Back | Back | Back |
Radiography | + | + | + | + | +/− | +/− | + | |
CT | + | + | + | + | ||||
MRI | + | + | + | + | + | + | + | + |
Bone scan with SPECT | + | + | + | + | ||||
Bone scan with SPECT/CT | + | + | + | + | + | + | + | + |
The major goal of bone scintigraphy is to establish whether the patient’s pain is related to an active bony process. Gates and McDonald argued that a normal bone scan effectively excludes a bony-based lesion (Gates and Mc Donald 1999). When bone pathology is present, nuclear scintigraphy has a proven role in the identification of a number of conditions including facet joint disease or instability, sacroiliac disease, pseudoarthrosis, fracture, and post-operative infection (Table 12.4). In particular, bone scans have the potential to detect active bone remodelling, whereas corresponding radiographs may be normal or document past structural change in the joint (Okamoto 1995). For instance, the sacral insufficiency fracture represents a repetitive, prolonged muscular action on the bone that has not accommodated itself to the action, resulting in stress fractures. The use of SPECT in addition to CT helps determine the cause of lower back pain (Fig. 12.6).
Table 12.4
Indications of bone scintigraphy with SPECT/CT in spine-related trauma
Negative CT or radiographic results |
Focal neurologic deficit |
Immunosuppression, diabetes mellitus |
Significant cumulative traumata |
Duration more than 6 weeks |
Fig. 12.6
A veteran female athlete with left pelvic pain. There is an old insufficiency fracture seen involving the left ala sacrum (round white marker) on the axial CT image. MIP 99mTc-MDP SPECT image shows slightly increased metabolic activity at the fracture site
The use of SPECT in bone scanning has improved the sensitivity and location capacity of these lesions by 20–50 % when compared to planar bone scan (Even-Sapir 2005) as is shown in Table 12.3.
Ghormley first coined the concept “facet joint syndrome” in 1933 when discussing alternate sources of lower back pain (Ghormley 1933). Lumbar spine facet joint pain may affect many patients with chronic lower back pain, with a wide estimation between 5 and 90 % (Cohen and Raja 2007). A small study using a computer algorithm to fuse the SPECT and CT data demonstrated an improved ability over SPECT alone in differentiating activity between L4/L5 and L5/S1 facet joints (McDonald 2007).
12.4.2 Cervicalgia and Cervicobrachialgia
Cervical spine strains and sprains frequently occur as a result of a whiplash injury, which often occurs as the result of motor vehicle accidents, falls, sports-related accidents, or other traumatic events that cause a sudden jerk of the head and neck (Rodrigo and Leonardo Oliveira 2006). The intensity of athletic competition has led to a large number of injuries that result in neck (cervicalgia) or upper limb pain (cervicobrachialgia), a situation made worse by the heavy backpacks among school-going adolescents and young athletes. Most injuries are a result of muscle strain or physical therapy. In older patients predominant arm pain (brachialgia) is related to mechanical pressure and inflammation of the involved nerve roots which is likely attributed to bone proliferation related to degeneration.
In many conditions, such as suspected infection or suspected acute osteoporotic crush fracture, MRI is the investigation of choice. CT is highly accurate for assessment of bone lesions such as suspected tumours or pars interarticularis defects. Bone scintigraphy with SPECT/CT is useful in distinguishing between abnormalities that are caused by fractures of the pars and other focal areas of increased activity that include facet joint osteoarthritis (Elster 1989).
Bone scintigraphy is also indicated to exclude spinal metastases, when there is a known primary tumour or a suspected pars interarticularis fracture for which changes may be difficult to see on plain radiographs, particularly in young patients with subtle stress fractures (Table 12.5). The majority of patients with non-specific cervicalgia show improvement of symptoms within 12 months. In this group there is value in identifying those in whom the cause is active facet arthropathy, since a corticosteroid injection to the culprit joints can hasten their symptomatic recovery (Fig. 12.7). SPECT/CT imaging is the ideal investigation in this group, given the additive information derived from the combination of functional and structural changes obtained.
Table 12.5
Differential diagnosis of cervicalgia and the diagnostic imaging tools that may be indicated
Evaluation | Neck strain | Degenerative disc disease | Myelopathy | Spondyloarthropathy | Tumour | Metabolic | Infection |
|---|---|---|---|---|---|---|---|
Predominant pain | Neck | Neck | Neck | Neck | Neck | Neck | Neck |
Radiography | + | +/− | + | +/− | + | +/− | |
CT | + | + | +
Related posts:Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|