Injury to cord, cranial nerve 12, C1 and C2 roots

• Vertebral artery (VA) injury primarily from screw placement (4%)
 If intraoperative injury to dominant VA occurs, attempts should be made to control bleeding and repair injury
If intraoperative injury to dominant VA occurs, attempts should be made to control bleeding and repair injury
If intraoperative injury to dominant VA occurs, attempts should be made to control bleeding and repair injury


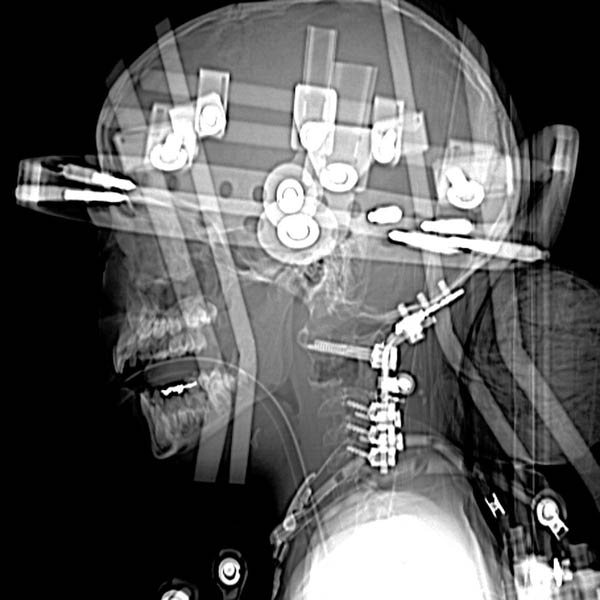

 was used as a scaffold for bony fusion. Occipital hardware is partially visible
was used as a scaffold for bony fusion. Occipital hardware is partially visible  , and gas is present in resection site
, and gas is present in resection site  .
.
 . The left vertebral artery (VA) was coil embolized after verifying that the right VA was patent.
. The left vertebral artery (VA) was coil embolized after verifying that the right VA was patent.
 .
.PRE-PROCEDURE
Indications





• Symptoms
 Cord and brainstem compression with respiratory distress, pain, cranial nerve dysfunction, paresis and paralysis, sudden death
Cord and brainstem compression with respiratory distress, pain, cranial nerve dysfunction, paresis and paralysis, sudden death




Cord and brainstem compression with respiratory distress, pain, cranial nerve dysfunction, paresis and paralysis, sudden deathRelated posts:


Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
