Chapter 12 Ocular Inflammatory Diseases

Introduction
Uveitis comprises a large group of inflammatory eye diseases involving the iris, ciliary body and choroid. The incidence of uveitis in the United States has been reported to be as high as 52.4/100 000 person-years in large population-based studies.1 Several classification schemes currently exist, based on etiology (infectious and non-infectious), clinical course (acute, chronic, and recurrent), anatomy (primary site of inflammation), and histopathology (granulomatous or nongranulomatous). Unique ultrasonography features may aid in the diagnosis of certain inflammatory conditions, such as toxocariasis.
Anterior uveitis
Anterior uveitis is the most common form of uveitis, accounting for approximately 90% of the cases. The inflammation is localized predominantly in the iris and pars plicata of the ciliary body, associated with a breakdown of the blood–aqueous barrier and increased aqueous protein and cells. The classic presentation of acute anterior uveitis is the sudden onset of pain, photophobia and redness, which may be accompanied by a decrease in visual acuity. There are numerous causes of anterior uveitis, including non-infectious disorders, such as sarcoidosis, Reiter’s syndrome, HLA B27 related iridocyclitis, inflammatory bowel disease, juvenile rheumatoid arthritis; as well as infectious conditions, related to agents such as herpesvirus and varicella-zoster virus.2
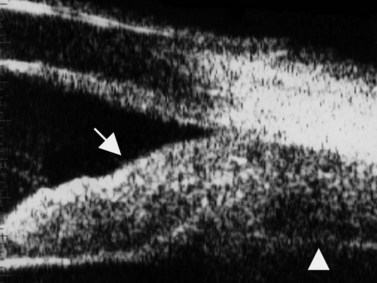
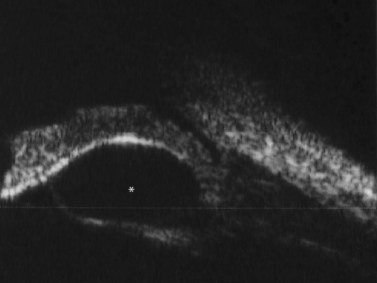
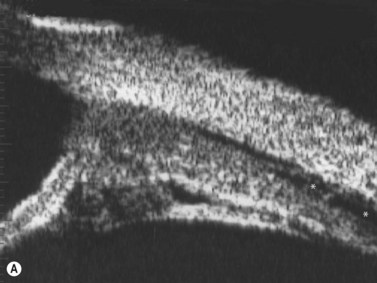
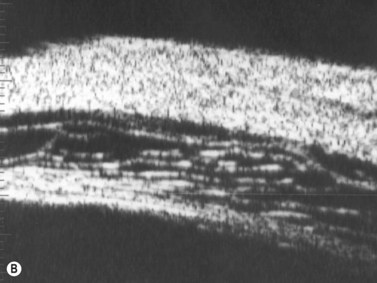
Although slit-lamp examination is sufficient to provide the diagnosis in the majority of cases, the use of ultrasound biomicroscopy (UBM) may disclose information on morphologic features of the anterior segment of the eye, not observed on clinical examination. Features that may be demonstrated by UBM include edema of the iris and ciliary body, demonstrating an irregular pattern of hyporeflectivity, and the presence of exudates adjacent to the ciliary body, as well as the vitreous base (Figure 12.1). Formation of cysts within the posterior iris and ciliary body epithelium at the iridociliary junction has also been described, more commonly related to nongranulomatous uveitis (Figure 12.2).3 A study by Peizeng et al reported that inflammatory changes could still be detected by UBM at 6 weeks after onset of uveitis, when the slit-lamp examination was unremarkable, indicating the need for further treatment, despite the disappearance of inflammatory cells from the anterior chamber.4
Intermediate uveitis
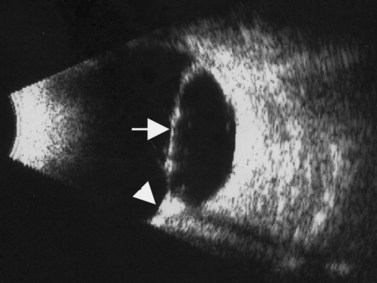
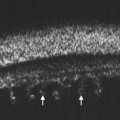
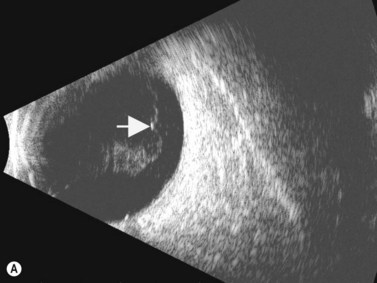
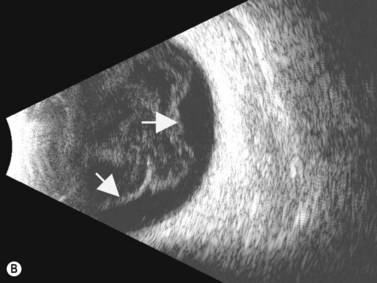
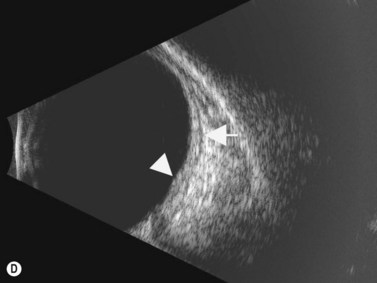
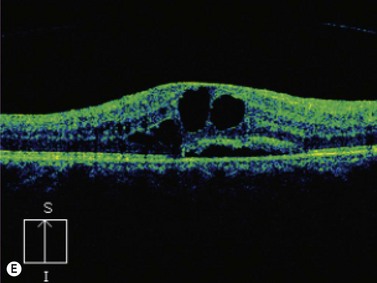
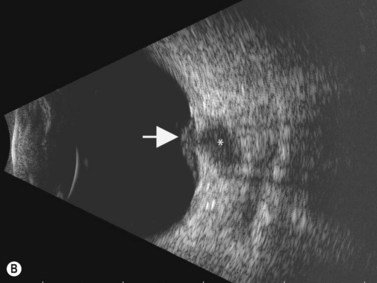
The Standardization of Uveitis Nomenclature (SUN) Working Group defines intermediate uveitis as the subset of uveitis where the primary site of inflammation is the vitreous (Figure 12.3). It may be associated with infections, such as Lyme disease, syphilis and tuberculosis, or other non-infectious conditions, such as sarcoidosis and multiple sclerosis. Inflammatory cells may aggregate in the vitreous (snowballs). In addition, exudates may be present in the pars plana (snowbanks), usually inferiorly and associated with more severe disease.5 These exudates are identified on UBM examination as highly reflective clumps of opacities adjacent or adherent to the pars plana (Figure 12.4).
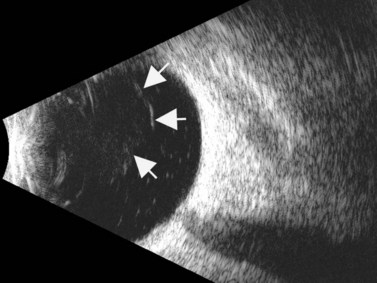
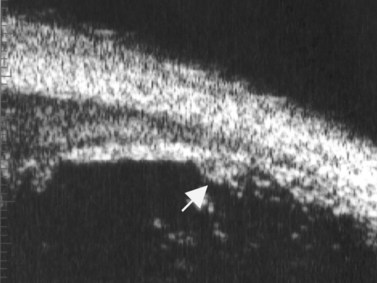
Figure 12.4 Pars planitis. UBM demonstrating white exudates, or “snowbanks” (arrow) over thickened pars plana.
Direct visualization of the posterior pole may be limited in the presence of opaque media. Anatomical structures mostly affected by intermediate uveitis are often not readily visible on funduscopy. The presence of pathological structures such as spotted or membranous vitreous condensations, ciliary body detachment and vitreoretinal adhesions have been documented by ultrasonography (Figure 12.5).6 In a study by Häring et al UBM demonstrated pathological lesions in almost 70% of cases of intermediate uveitis. Lesions appeared as vitreous condensations or membranes of various configurations and extent, located over the peripheral retina and pars plana, and sometimes also extending towards the pars plicata. In 34.6% of eyes enrolled in the study, UBM disclosed pathological lesions not identified on ophthalmoscopy with scleral indentation.7 Additionally, a good correlation of the activity of pars planitis evaluated by UBM as compared to that by indirect ophthalmoscopy has been demonstrated.8 Therefore, UBM can be helpful in the management of patients, grading severity and guiding treatment decisions (Figure 12.6).
Posterior uveitis
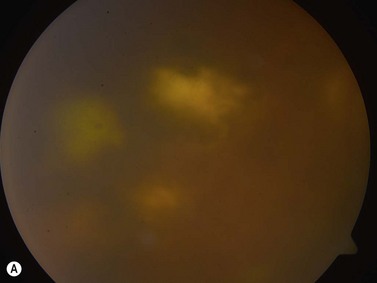
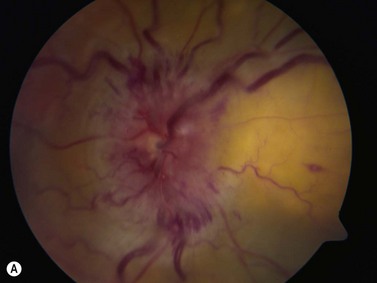
The primary site of inflammation in posterior uveitis is the choroid, the retina or both. Inflammatory cells may be seen diffusely throughout the vitreous cavity. Many posterior uveitis syndromes are the result of an underlying infection, including toxoplasmosis, syphilis, toxocariasis, tuberculosis, cytomegalovirus retinitis and ocular histoplasmosis syndrome. Non-infectious etiologies include disorders such as sarcoidosis, white dot syndromes and collagen vascular diseases (Figure 12.7).9 The signs and symptoms of posterior uveitis are variable, depending on the location and extent of inflammation.


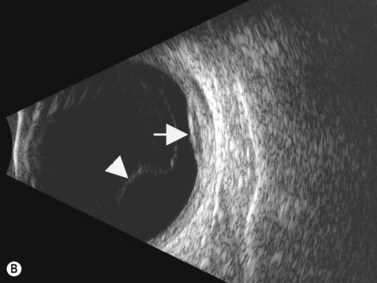
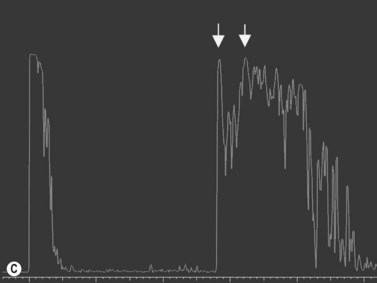
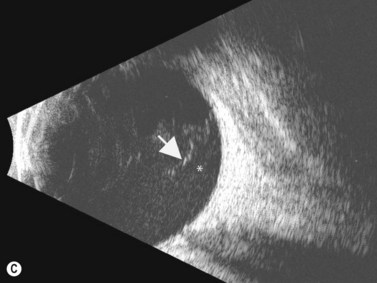
Ultrasonography can be a very useful tool, particularly in cases in which the media is not clear, secondary to severe vitritis or vitreous hemorrhage. See Clip 12.1A,B 9 Specific ultrasonographic findings may aid in the diagnosis of certain conditions. Characteristic pseudocystic degeneration of the peripheral vitreous has been described in patients with ocular toxocariasis.10 Other ultrasonographic features that can be observed in toxocariasis include mildly to moderately elevated granulomatous lesions that can be calcified, vitreous membranes extending from the granulomatous lesion to the posterior pole and posterior tractional retinal detachment or retinal fold (Figure 12.8). A retrospective study by Hercos et al reported ultrasonographic findings in patients with ocular toxoplasmosis. The most frequent features were intravitreal punctiform echoes, thickening of the posterior hyaloid, partial or total posterior vitreous detachment and focal retinochoroidal thickening (Figure 12.9).11
See Clip 12.1A,B 9 Specific ultrasonographic findings may aid in the diagnosis of certain conditions. Characteristic pseudocystic degeneration of the peripheral vitreous has been described in patients with ocular toxocariasis.10 Other ultrasonographic features that can be observed in toxocariasis include mildly to moderately elevated granulomatous lesions that can be calcified, vitreous membranes extending from the granulomatous lesion to the posterior pole and posterior tractional retinal detachment or retinal fold (Figure 12.8). A retrospective study by Hercos et al reported ultrasonographic findings in patients with ocular toxoplasmosis. The most frequent features were intravitreal punctiform echoes, thickening of the posterior hyaloid, partial or total posterior vitreous detachment and focal retinochoroidal thickening (Figure 12.9).11