Chapter 16 Ocular Trauma

Introduction
Ocular trauma is a major cause of vision loss, particularly among younger patient populations. Traumatic injuries also represent one of the more difficult clinical examinations due to the severe pain associated with such injuries. Since examination of the traumatized globe may be limited to only a brief clinical examination secondary to pain, it is important that the echographer be aware of the various types of pathologic changes that are most likely to occur with certain types of traumatic injuries. Vitreoretinal involvement is present in nearly 50% of all severe eye injuries secondary to blunt or penetrating trauma.1
Clinical examination of the posterior segment can, however, be limited in such cases by factors related to the injury. Coexisting anterior segment injury can result in hyphema or corneal edema and opacification. Traumatic posterior segment pathology, such as vitreous hemorrhage can limit the diagnostic information obtained from clinical examination. In such cases, B-scan ocular ultrasonography has been shown to yield valuable diagnostic and prognostic information to define the nature of the pathology and guide management.2,3 In a review of 154 eyes with various posterior segment disorders for which ultrasound was ordered at one institution, it was reported that ultrasonography data made an impact on disease diagnosis or management in 83% of cases and were “pivotal” in 14% of cases.4 Although ultrasonography (B-scan and ultrasound biomicroscopy) is a valuable adjunct to management of trauma, one must exercise caution that it alone does not guide surgical intervention. Ultrasonography must be used in conjunction with other imaging modalities and the clinical examination, with particular attention to intraocular pressure.
Anterior segment
In the setting of trauma, ultrasound can be used to assess the anterior segment in patients with hyphemas or corneal opacification. In the setting of hyphema, an ultrasound can be instrumental in demonstrating the presence or absence of a clot and the depth of the anterior chamber.5
Angle trauma
Ultrasound can also be utilized to evaluate delicate angle anatomy in order to examine for iridodialysis, angle recession, or cyclodialysis. The examination for a cyclodialysis cleft is especially important in a patient with persistent hypotony following trauma. The sequelae of cyclodialysis include shallow anterior chamber, cataract, retinal and choroidal folds, hypotonus maculopathy, and loss of vision in cases of prolonged hypotony.6 Clinically, a cyclodialysis cleft can be difficult to detect if the anterior chamber is shallow and there is corneal edema or anterior chamber hyphema (Figure 16.1). Ultrasound biomicroscopy (UBM) is a safe, accurate and noninvasive diagnostic tool in the diagnosis of cyclodialysis clefts (Chapter 4).7
Ultrasonography can also be instrumental in the evaluation of dislocated corneal grafts following Descemet stripping with endothelial keratoplasty (DSEK).8 In fact, ultrasonography can be useful in the evaluation of post-traumatic eyes that have undergone any type of endothelial keratoplasty, as donor dislocation can occur after any type of endothelial keratoplasty procedure, including posterior lamellar keratoplasty (PLK), deep lamellar endothelial keratoplasty (DLEK), or DSEK, because the donor tissue is not secured with any sutures.9
Lens dislocation
Blunt trauma can lead to the subluxation or dislocation of the crystalline lens or intraocular lens implants through the disruption of zonular fibers. Lens dislocation or subluxation has been reported from several sources of blunt trauma, including seizure-related injury,10 airbag deployment,11 paint-ball injuries,12,13 bottle corks,14 and plastic cord-related injuries.15–17 Subluxed lenses often can be identified with the slit-lamp, and subtle cases can be distinguished by looking for associated signs, such as iridodonesis and phakodonesis. Complete dislocation of an intraocular lens or crystalline lens can be identified in the posterior segment through indirect ophthalmoscopy, although dislocation into the anterior chamber or even the subconjunctival space also can occur.18–20
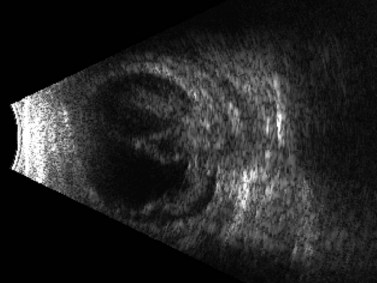
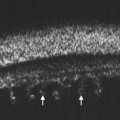
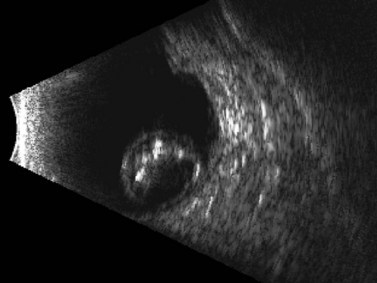
In cases in which other trauma-associated pathology, such as corneal opacification, hyphema, and vitreous hemorrhage, preclude posterior segment examination, dynamic ultrasonography can help to determine the position of the dislocated lens. On B-scan, a posteriorly dislocated crystalline lens appears as an oval-shaped, highly reflective mass that can be misdiagnosed as an intraocular tumor without careful attention to internal reflectivity and mobility (Figure 16.2). See Clip 16.1 A traumatically displaced intraocular lens appears as a highly reflective linear body with marked reverberations along the echoic plane and two focal areas of reverberations corresponding to the intraocular lens haptics (Figure 16.3). Management options for crystalline lens injury range from observation in cases of mild subluxation without significant traumatic cataract to lens removal using vitrectomy techniques in cases of complete posterior dislocation.21 Finally, ultrasonography can be used to determine whether a lens (either crystalline or pseudophakic) has been extruded from the eye altogether.
See Clip 16.1 A traumatically displaced intraocular lens appears as a highly reflective linear body with marked reverberations along the echoic plane and two focal areas of reverberations corresponding to the intraocular lens haptics (Figure 16.3). Management options for crystalline lens injury range from observation in cases of mild subluxation without significant traumatic cataract to lens removal using vitrectomy techniques in cases of complete posterior dislocation.21 Finally, ultrasonography can be used to determine whether a lens (either crystalline or pseudophakic) has been extruded from the eye altogether.
Posterior segment
Rhegmatogenous retinal detachment
Trauma is the most common cause of retinal detachment in children and may play a role in approximately 10% of retinal detachments overall.1,22 Retinal detachment after blunt trauma may develop as a result of retinal dialysis, flap tears, operculated tears, macular hole, and giant retinal tears through rapid compression–decompression forces that result in transient anteroposterior shortening and equatorial elongation of the globe. It is estimated that 70% of hemorrhagic posterior vitreous detachments may have an associated retinal tear,23 and this association is likely even greater in the specific setting of trauma. Peripheral tears also can occur as a result of trauma-induced vitreous detachment.
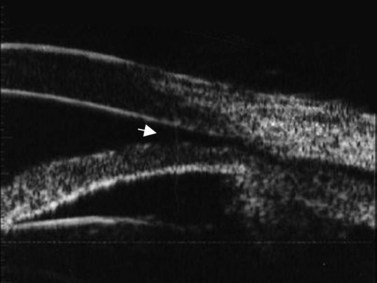
Although indirect ophthalmoscopy remains the technique of choice for diagnosing a retinal tear or detachment in this setting, ultrasonography can be of value when the view of the posterior segment is obscured by dense vitreous hemorrhage (Chapter 10). A small, peripheral retinal tear appears as a focal, highly reflective flap on B-scan (Figure 16.4). The posterior vitreous is usually thickened and partially detached but remains adherent to the retina at the location of the tear. In addition to the dense, vitreous hemorrhage, this adhesion sometimes can make the diagnosis of a peripheral retinal tear difficult and can lead to false-negative results. In a review of 106 eyes undergoing ultrasonography for dense vitreous hemorrhage, only 44% of retinal tears were diagnosed accurately.24 To maximize diagnostic sensitivity, examination of a suspicious area at a low gain and focally guided ocular movements to access flap mobility are essential.
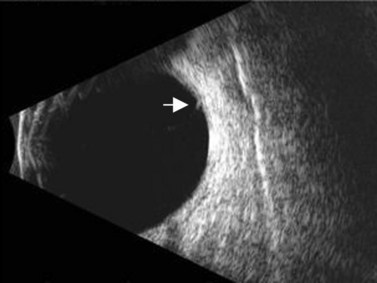
Figure 16.4 Peripheral retinal tear. Longitudinal B-scan at a low gain displays small, highly reflective flap (arrow).
Reproduced with permission from: Dadgostar H, Ventura ACM, Hayden BC. Posterior segment trauma. Ultrasound Clin 2008; 3:267–272.
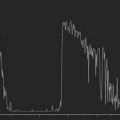
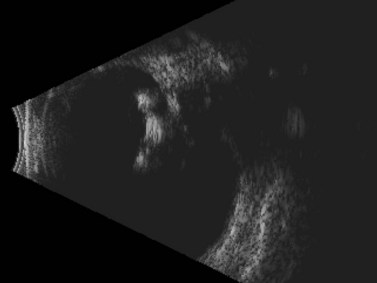
Because many cases involve younger patients with formed vitreous, the progression of a tear or dialysis to a detachment may take weeks to months;25 however, giant retinal tears have a much higher chance of progressing rapidly to retinal detachment.26 Giant retinal tears present on ultrasonography as highly reflective, discontinuous, rope-like membranes within the vitreous space (Figure 16.5). In the presence of dense hemorrhage, standardized diagnostic A-scan is an essential tool in the differentiation of a discontinuous, thickened posterior vitreous detachment from a giant retinal tear (Figure 16.6).
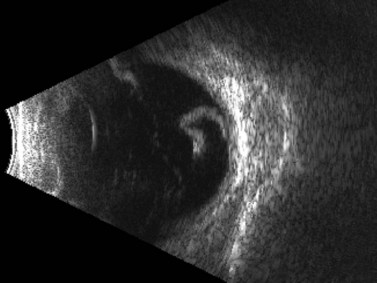
Figure 16.5 Giant retinal tear. Transverse view shows discontinuous, folded, hyperechoic retina.
Reproduced with permission from: Dadgostar H, Ventura ACM, Hayden BC. Posterior segment trauma. Ultrasound Clin 2008; 3:267–272.
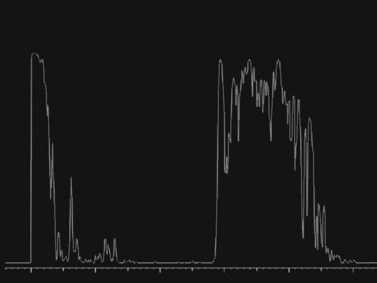
Figure 16.6 Diagnostic A-scan directed perpendicular to the retinal tear shows a 100% spike at tissue sensitivity.
Reproduced with permission from: Dadgostar H, Ventura ACM, Hayden BC. Posterior segment trauma. Ultrasound Clin 2008; 3:267–272.
Some injuries such as giant retinal tear and detachment may appear “flat” on B-scan when in fact the retina is folded over under dense hemorrhage. For this reason, the intraocular pressure becomes a valuable characteristic in determining which eyes should be explored. In cases of low intraocular pressure even after primary closure, exploration within the first 1–2 weeks should be considered. In addition, any suspicion of retinal tear in cases of dense vitreous hemorrhage warrant exploration by vitrectomy and scleral buckle because of the high risk of proliferative vitreoretinopathy.27
Penetrating ocular injury that tears the retina directly typically does not result in immediate rhegmatogenous detachment. In these cases, a delayed combined tractional and rhegmatogenous detachment often results from intraocular fibrovascular proliferation that originates from the site of injury (Figure 16.7).28 As demonstrated in animal models, this progressive proliferative vitreoretinopathy ultimately can lead to total retinal detachment, hypotony, and phthisis, if untreated.29,30