AORTA AND INTERRUPTED
AORTIC ARCH
 COARCTATION OF THE AORTA
COARCTATION OF THE AORTA
Definition, Spectrum of Disease, and Incidence
Coarctation of the aorta involves narrowing of the aortic arch, typically located at the isthmic region, between the left subclavian artery and the ductus arteriosus (Fig. 12-1). Alternatively, coarctation of the aorta may involve a long segment of the aortic arch, termed tubular hypoplasia of the aortic arch. Coarctation of the aorta is a common anomaly, found in about 5% of newborns with congenital heart disease (1). It occurs more commonly in boys, with a male-to-female ratio of 1.27 to 1.74 (2,3). Coarctation of the aorta has a fairly high recurrence risk, between 2% and 6% for a previously affected child and 4% for an affected mother (4,5). Chromosomal and extracardiac abnormalities are common associations with coarctation of the aorta (6). The embryologic origin of coarctation of the aorta is complex and not well understood, with two proposed concepts; the ductus tissue theory proposes that aortic constriction is due to migration of ductal smooth muscle cell into the aorta (7), whereas the hemodynamic theory proposes that coarctation results from reduced flow through the aortic arch in fetal life (8). Coarctation of the aorta can be classified as simple when it occurs without important intracardiac lesions and complex when it occurs in association with significant intracardiac pathology. When associated with hypoplastic left heart syndrome and aortic atresia, hypoplastic aortic arch should not be classified as coarctation of the aorta but rather as part of the main cardiac anomaly. Table 12-1 lists cardiac malformations that may include
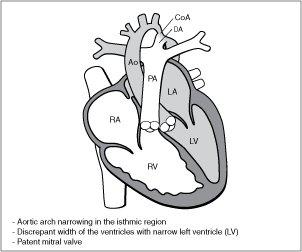
Figure 12-1. Coarctation of the aorta. RA, right atrium; RV, right ventricle; LA, left atrium; PA, pulmonary artery; Ao, aorta; DA, ductus arteriosus; CoA, coarctation of the aorta.
| TABLE 12-1 | Cardiac Anomalies That May Include Coarctation of the Aorta or Tubular Aortic Hypoplasia as Part of the Abnormalities |
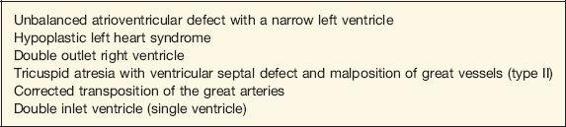
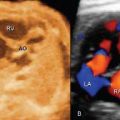
aortic coarctation or tubular aortic hypoplasia as part of the main cardiac anomaly. Figure 12-2 demonstrates coarctation of the aorta in an anatomic specimen of a fetal heart.
Ultrasound Findings
Gray Scale
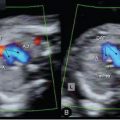
Coarctation of the aorta is often associated with an abnormal four-chamber view, where the left ventricle appears narrow when compared to the right ventricle (9–11) (Fig. 12-3). The right ventricular–to–left ventricular width ratio, reported as 1.19 in normal fetuses, is 1.69 in fetuses with coarctation of the aorta (12). Conversely to hypoplastic left heart syndrome, in coarctation of the aorta the contractility of the left ventricle is normal and the mitral valve is patent. The five-chamber view shows the arising aorta with a generally normal diameter. The aortic root can be narrow on occasions, especially when a perimembranous ventricular septal defect and/or aortic stenosis are present. In the three-vessel-trachea view, the diameter of the transverse aortic arch is narrow when compared to the main pulmonary artery (12), and this narrowing of the transverse aortic arch is most impressive in the isthmus region (Fig. 12-4). In the diagnosis of aortic coarctation, the three-vessel-trachea view, depicting the great vessel disproportion, is more specific than ventricular disproportion alone noted on a four-chamber view. Once coarctation of the aorta is suspected in the transverse planes (four-chamber and three-vessel-trachea views), a longitudinal view of the aortic arch should be attempted. In this
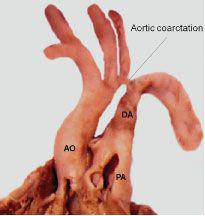
Figure 12-2. Anatomic specimen of coarctation of the aorta in a fetal heart showing aortic narrowing at the aortic isthmus (labeled aortic coarctation). AO, aorta; PA, pulmonary artery; DA, ductus arteriosus.
Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


