The oral cavity, commonly known as “mouth”, is a part of the digestive system and also helps in breathing. It is situated anteriorly on the face, below the nasal cavities, and extends from the oral fissure or the opening between the lips anteriorly to the oropharyngeal isthmus posteriorly. It has a complex anatomy consisting of different sites and subsites and is a challenging area for radiological diagnosis. There are many diseases that can affect the oral cavity, cancer being the commonest and most important disease of this region. The entire mucosa of the oral cavity can be optimally visualized at clinical examination, and the patient is generally referred for imaging after a diagnosis has been made at biopsy in suspected cancers. CT and MRI contribute significantly to the diagnostic evaluation of submucosal masses and deeper extensions of cancerous lesions, significantly impacting their prognosis and therapeutic options.
Anatomy
Oral cavity is broadly divided into a central larger portion called “oral cavity proper” and an outer lateral portion called the “vestibule”. Oral cavity proper is bound superiorly by the hard palate, laterally by the upper and lower alveolus covered by the gingival mucosa and inferiorly by the mylohyoid muscle. It opens posteriorly into the oropharynx. Vestibules are mucosa lined spaces that extend from the lips anteriorly to the retromolar trigone (RMT) posteriorly and are bound by the cheeks laterally and the gums and teeth posteriorly and medially. They are bound superiorly and inferiorly by the superior and inferior gingivobuccal sulci or gutters, respectively. All the surfaces of the oral cavity structures are covered with keratinizing stratified squamous epithelium along with minor salivary gland rests.
The various anatomical subsites of the oral cavity are enlisted in Box 3.8.1. Refer Figs. 3.8.1–3.8.6 for the CT and MRI anatomy of the oral cavity.
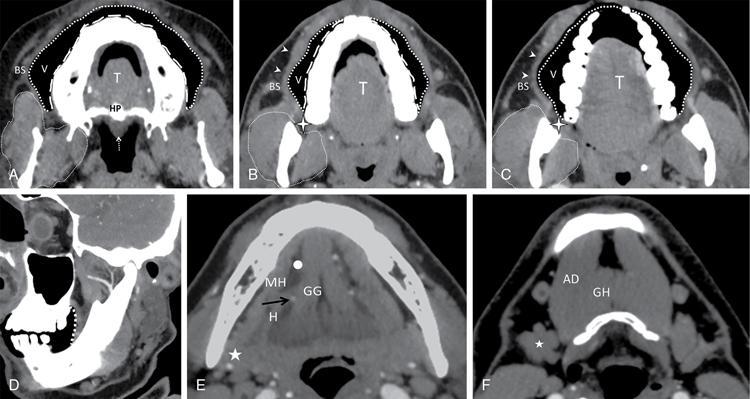
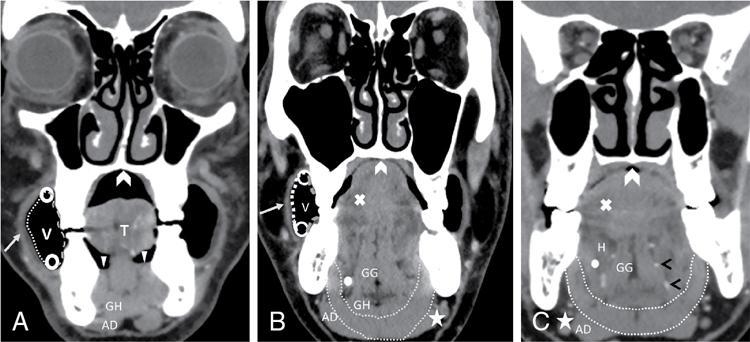
Fig. 3.8.1CECT sections of oral cavity obtained with puffed cheek technique in axial and oblique sagittal reformation depicting normal anatomy. (A) Superior section showing the dorsum of the tongue (T), small portion of the hard palate (HP) and the soft palate (white dashed arrow). Air distended vestibule is seen (V) bordered by the buccal mucosa laterally (thick white round dotted line) and the gingival mucosa medially (white long dashed line). Note the masticator space posterolateral to the gingivobuccal region (enclosed by small white dotted line). (B) The dorsum of the tongue (T) is seen. Air distended vestibule is seen (V) bordered by the buccal mucosa laterally (thick white round dotted line) and the gingival mucosa medially (white long dashed line). The buccinator muscle (small white arrowheads) is seen better in this section stretched around the distended vestibule and forms the medial boundary of the buccal space (BS). Note the masticator space (enclosed by small white dotted line) posterolateral to the gingivobuccal region and the buccal space. The upper limit of the retromolar trigone is seen at the level of the maxillary tuberosity (black outlined white star). (C) The dorsum of the tongue (T) is seen. Air distended vestibule is seen (V) bordered by the buccal mucosa laterally (thick white round dotted line) and the gingival mucosa medially (white long dashed line). The buccinator muscle (small white arrowheads) is seen better in this section stretched around the distended vestibule and forms the medial boundary of the buccal space (BS). The retromolar trigone is seen at the level of the maxillary tuberosity (black outlined white star). The masticator space enclosed by small white dotted line is seen just posterolateral to the retromolar trigone. (D) Oblique sagittal reformation shows the retromolar trigone (dotted white line) which is the mucosal fold in the area posterior to the mandibular last molar extending along the ascending ramus of mandible up to the maxillary last molar on either side. (E) Axial section at the level of the floor of the mouth shows the paired genioglossus (GG) muscles that are paramedian in position. The hyoglossus muscle (H) is seen lateral to the genioglossus (GG) and further lateral are the mylohyoid muscles (MH). Mylohyoid muscle (MH) divides the sublingual space (white circle) from submandibular space (white star). Within the sublingual space, the lingual artery is seen medial to the hyoglossus muscle (black arrow) and the lingual vein and submandibular duct are seen lateral to the hyoglossus muscle. (F) A very caudal section shows the anterior belly of digastric muscles (AD) and the geniohyoid muscles (GH) that support the mylohyoid sling. The submandibular glands are seen (white star).
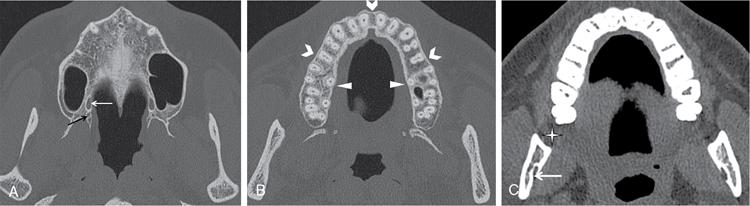
Fig. 3.8.2Axial and oblique sagittal reformatted CT sections in bone window. CT provides excellent assessment of cortical bone and osseous neural foramina. (A) Section at the level of hard palate shows greater palatine foramen (white arrow) and lesser palatine foramen (black arrow). These serve as important pathways for perineural spread of cancers of the hard palate along the greater and lesser palatine nerves. (B) Axial section at the level of superior alveolus shows the buccal (white chevrons) and lingual (white arrowheads) cortices of maxilla. (C) Axial section at the level of the retromolar trigone (white star) shows the close relationship of the RMT with the mandibular ramus. The white arrow points to the mandibular foramen. (D) Oblique sagittal reformation shows the entire extent of the inferior alveolar canal (dashed black arrows) in the body of the mandible. It starts from the lingual side of mandibular ramus at the mandibular foramen (white arrow in C), continues on buccal surface of body of mandible and ends at mental foramen adjacent to second mandibular premolar tooth. It is again an important anatomical pathway for perineural spread of cancers of the floor of mouth. (E) Axial section at the level of inferior alveolus showing the buccal (white chevrons) and lingual (white arrowheads) cortices of mandible.
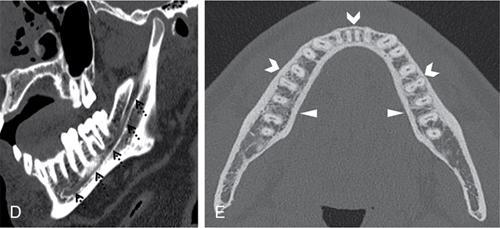
Fig. 3.8.3Axial T2 weighted MRI images of oral cavity from superior to inferior levels depicting normal anatomy: (A) The dorsum of the tongue (T) shows the intrinsic muscles (white cross). Buccal mucosa is laterally lined by buccinator muscle (black arrowheads) that forms the medial boundary of the buccal space (BS). Further anterolaterally is seen the levator anguli oris muscle (white arrow). The retromolar trigone or RMT is seen behind the last molar (white star) and houses the pterygomandibular raphe PMR that provides attachment to the buccinator muscle (black arrowheads). The PMR forms the anterior boundary of the pterygomandibular space (small dotted white line) located between the medial pterygoid muscle and the ramus of mandible. The masticator space (dashed white line) is seen posterolateral to the retromolar trigone. (B) The dorsum of the tongue (T) shows the intrinsic muscles (white cross) and the genioglossus muscles (GG). Buccal mucosa is laterally lined by buccinator muscle (black arrowheads) that forms the medial boundary of the buccal space (BS). Further anterolaterally is seen the levator anguli oris muscle (white arrow). The retromolar trigone or RMT is seen behind the last molar (white star) and houses the pterygomandibular raphe PMR that provides attachment to the buccinator muscle (black arrowheads). The masticator space (dashed white line) is seen posterolateral to the retromolar trigone. The pterygomandibular space (small dotted white line) and ramus of mandible (curved white arrow) are seen within the masticator space. The thick white dotted line passes through the anterior margin of the ramus of mandible and forms an imaginary plane of demarcation between the oral and oropharyngeal portions of the tongue. (C) Slightly caudal section shows the styloglossus muscles (white arrowhead) in the tongue. Note the depressor anguli oris (white arrow), the buccinator (black arrow heads), the genioglossus (GG) and the masticator space (white dashed line). (D) Axial section through the floor of mouth shows the paired genioglossus (GG) muscles that are paramedian in position. The hyoglossus muscle (H) is seen lateral to the genioglossus (GG) and further lateral are the mylohyoid muscles (MH). Mylohyoid muscle (MH) divides the sublingual space (dotted white line contour) from submandibular space (white line contour). Note the sublingual gland (white circle) and the submandibular gland (white star). Within the sublingual space, the lingual artery is seen medial to the hyoglossus muscle (white arrow) and the lingual vein and submandibular duct are seen lateral to the hyoglossus muscle. (E) A very caudal section shows the anterior belly of digastric muscles (AD) and the geniohyoid muscles (GH) that support the mylohyoid sling. The submandibular glands are seen (white star).
Fig. 3.8.4Coronal CECT sections of oral cavity obtained with puffed cheek technique from anterior to posterior direction depicting normal anatomy: (A) The air distended central oral cavity proper contains the tongue (T) and is bound superiorly by the mucosa lining the hard palate (^) and caudally by the mucosa of the floor of mouth (white arrowheads). The air distended vestibules (V) are seen medially bound by the gingival mucosa (grey dashed line), laterally by buccal mucosa (white dotted line) and the superior and inferior gingiva-buccal sulci (white circles). The buccinator muscle is stretched around the buccal mucosa (white arrow). Note the anterior belly of digastric (AD) and geniohyoid (GH) muscles. (B) Coronal image posterior to (A) shows the mylohyoid sling (white dotted line), genioglossus muscle (GG), the geniohyoid muscle (GH) and intrinsic muscles of tongue (white cross). Note the fat density of the sublingual space (white dot) superior to the mylohyoid sling which separates it from the inferior submandibular space (SMS, white asterisk). The anterior belly of digastric muscle (AD) is seen below the mylohyoid muscle forming its support in SMS. Note the buccinator muscle stretched along the buccal mucosa (white arrow) and the hard palate forming the roof of the oral cavity (^). (C) Coronal section further posteriorly shows the mylohyoid sling (dotted white line), the genioglossus muscles (GG), hyoglossus muscles (H) and intrinsic muscles of tongue (white cross). Hyoglossus muscle separates the sublingual space (white circle) with lingual artery (black open arrowheads) seen medial to it. Hard palate (^), anterior belly of digastric muscle (AD) and submandibular space (white asterisk).
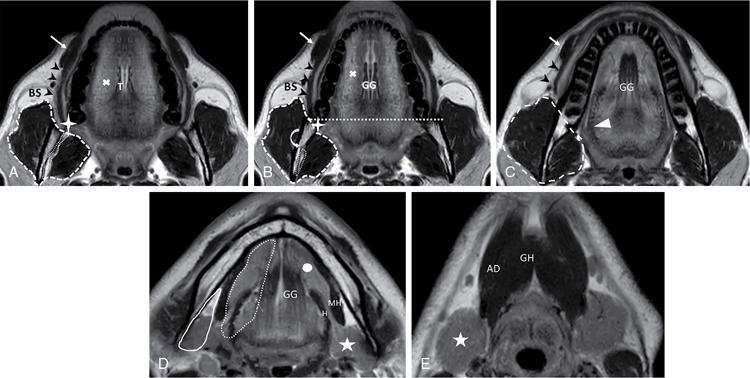
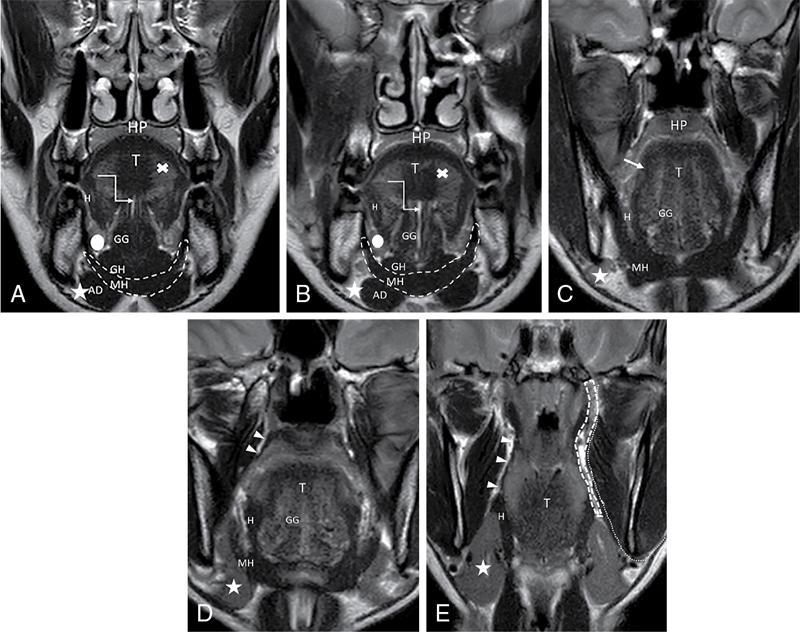
Fig. 3.8.5Coronal T2 weighted MRI images of oral cavity from anterior to posterior direction depicting normal anatomy. Note the exquisite depiction of the soft tissue anatomy on T2 weighted MRI images without fat suppression. (A) The genioglossus (GG) and geniohyoid (GH) muscles are seen in paramedian location separated by midline lingual septum (white elbow arrow). The hyoglossus (H) inserts onto the lateral surface of tongue. The intrinsic muscles (white cross) are seen. The mylohyoid sling (MH) forms the floor of the mouth and separates the sublingual space (white circle) from the submandibular space (white asterisk). The anterior belly of digastric muscle (AD) is a component of the submandibular space and supports the mylohyoid sling (MH). Superiorly the oral cavity is limited by hard palate (HP). (B) The genioglossus (GG) and geniohyoid (GH) muscles are seen in paramedian location separated by midline lingual septum (white elbow arrow). The hyoglossus (H) inserts onto the lateral surface of tongue. The intrinsic muscles (white cross) are seen. The mylohyoid sling (MH) forms the floor of the mouth and separates the sublingual space (white circle) from the submandibular space (white asterisk). The anterior belly of digastric muscle (AD) is a component of the submandibular space and supports the mylohyoid sling (MH). Superiorly the oral cavity is limited by hard palate (HP). (C) The styloglossus muscle (white arrow) is seen merging with the hyoglossus muscle (H). The mylohyoid sling (MH) separates the floor of mouth from the submandibular space (white star). Hard palate (HP) forms the roof of the oral cavity. (D) The palatoglossus muscles (white arrow heads) are seen merging with the hyoglossus muscles (H). Note the genioglossus (GG), the mylohyoid sling (MH) and the submandibular gland (white star). (E) The palatoglossus muscles (white arrow heads) are seen merging with the hyoglossus muscles (H). Note the submandibular gland (white star). Masticator space is lined by white dotted line with the parapharyngeal space (white dashed line) seen medial to it which largely contain fat and neurovascular structures.
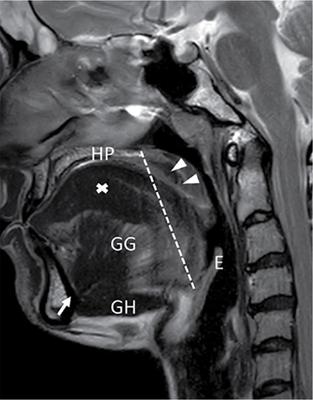
Fig. 3.8.6The muscular anatomy of the tongue is best seen on MRI images. Midline sagittal image shows the fan shaped genioglossus (GG) and flat geniohyoid (GH) muscles. They originate from superior and inferior aspects of the genial tubercle of mandible respectively (white arrow) and form the root of the tongue. The intrinsic muscles of the tongue (white cross) and palatoglossus (white arrowheads) are nicely seen on the sagittal MR image. Oral tongue is separated from the base of tongue by an oblique line (white dotted line) extending from the junction of hard palate (HP) and soft palate to the valleculae. The base of tongue has only the intrinsic muscles of the tongue. Epiglottis (E) is seen posterior to base of tongue.
The upper and lower lips are the anterior border of the oral cavity. The vermilion border is the junction and the sharp demarcation between the facial skin and the lip.
• Gingivobuccal mucosa
The upper and lower alveolar ridges contain the alveolar sockets for the teeth and are covered by the gingival mucosa. Medially, the upper alveolus transitions to the hard palate, while the lower alveolus transitions to the floor of the mouth. The upper alveolus extends posterosuperiorly to the maxillary tuberosity, and the lower alveolus continues posteriorly to the RMT. Lateral to each alveolus is the gingivobuccal sulcus, which is the transition of the gingival mucosa overlying the alveolus to the buccal mucosa. The buccal mucosa covers the inner aspect of the cheeks and lips. Lateral to buccal mucosa is the buccal space that further leads superiorly to the masticator space. Though these spaces are not components of the oral cavity, they are commonly involved by buccal cancers and hence a knowledge of their anatomical relationship with the gingivobuccal mucosa is important. The gingivobuccal mucosal space is normally collapsed, making it difficult to evaluate early cancers, and hence a “puffed-cheek” CT technique is used in their radiological evaluation. This is discussed under the section of “Protocols and Techniques for Examination” in the chapter on Diseases of the Oral Cavity.
• Retromolar trigone
RMT is a triangular mucosal fold overlying the area posterior to the mandibular last molar, extending along the ascending ramus of the mandible up to the maxillary last molar on either side. It is continuous with the buccal mucosa anterolaterally and the anterior tonsillar pillar of the oropharynx medially. Underneath the RMT is the pterygomandibular raphe (PMR) which is a fibrous band that connects the posterior mylohyoid line of mandible to the hamulus of the medial pterygoid plate. The PMR provides attachment to the buccinator and the superior constrictor muscles. Additionally, it forms the anterior boundary of the pterygomandibular fat space that is located between the medial surface of the ramus of the mandible and the medial pterygoid muscle and is actually a subspace within the masticator space. It contains the inferior alveolar nerve and vessels and is continuous anteriorly with the buccal fat space. Hence, the RMT has very close relationships with the buccal space, the pterygomandibular space and the masticator space.
It only follows naturally that the RMT serves as a junction box for spread of disease to and between the oral cavity, oropharynx, buccal space, pterygomandibular space and the masticator space.
At axial imaging, the RMT is seen in at least a few slices extending from the level of the mandibular to the maxillary last molar. Oblique reformations at MDCT allow for the visualization of the RMT in its full extent.
• Oral tongue
Oral tongue is the anterior two-third portion of the tongue. It is demarcated by the sulcus terminalis and the circumvallate papillae from the posterior third portion that is a part of the oropharynx. This demarcation is not visualized at imaging, and as a general guide, a line joining the anterior aspect of the mandibular rami on axial images may be used as the dividing line between these two portions. On a midsagittal image, a line dropped down from the junction of the hard and soft palates down to the glossoepiglottic junction is considered as the dividing plane between the oral and oropharyngeal tongue. It is important to differentiate these two regions since they are different embryologically and also the cancers in each of these portions behave differently from one other.
The tongue comprises intrinsic and extrinsic muscles. As the name suggests, intrinsic muscles are entirely within the tongue and are named in the direction in which they travel – superior longitudinal, inferior longitudinal, transverse and vertical. The superior longitudinal muscle is unpaired and seen just beneath the lingual mucosa. The other muscles are paired and interdigitate – they cannot be differentiated at imaging. The extrinsic muscles arise outside the tongue and include the genioglossus, hyoglossus, palatoglossus and styloglossus. Their attachments and important features are summarized in Table 3.8.1. The oral tongue itself is further divided into tip, root, dorsum, lateral border and the undersurface. The midline fibrofatty lingual septum divides the tongue into two halves.
Arises from the superior genial tubercle of mandible and fans out superiorly, interdigitating with intrinsic muscles of tongue. Inferiorly, it inserts onto the body of the hyoid bone.
It lies on each side of the paramedian plane.
Seen very well on axial, coronal and sagittal MRI
Forms the bulk of the oral tongue and is also an important component of the root of the tongue.
Hyoglossus
Arises from the body and greater horn of hyoid bone and inserts on the lateral surface of the tongue
Thin flat muscles that are lateral to the genioglossus muscles and lie in the sublingual space
It is the most important landmark to localize the neurovascular bundle of the tongue. It separates the lingual artery which is medial to it, from the lingual vein and main submandibular duct that are lateral to it.
Palatoglossus
Arises from the oral surface of soft palate and reaches the dorsolateral surface of the tongue to blend with the hyoglossus
Forms the anterior tonsillar pillar
Styloglossus
Arises from the styloid process and the stylomandibular ligament to traverse between the ICA and ECA and then blends with the hyoglossus on the lateral surface of the tongue
Inconsistently visualized at imaging
The lingual neurovascular bundle is formed by the lingual artery and veins, hypoglossal nerve and lingual nerve. Only the palatoglossus muscle receives motor supply from the vagus nerve. The hyoglossus muscle is the important landmark for locating these structures. The lingual artery is medial to the hyoglossus. At the anterior margin of the hyoglossus, it gives off the sublingual artery and then bends sharply upward toward the genioglossus muscle and runs along its lateral side close to the ventral surface of the tongue. The lingual nerve is lateral to the hyoglossus muscle. It twists around the submandibular duct and then enters the tongue. It is interesting to note that the midline lingual septum does not allow any anastomosis between the lingual artery of either side except at the tip.
The tongue has a rich lymphatic network. The lymph from the tip of the tongue drains to the submental nodes. Lymphatics from the outer third of the rest of the oral tongue drain into ipsilateral submandibular and jugulodigastric nodes.
The oral portion of the tongue has a fairly homogeneous appearance on CT, mainly that of muscle laced with fat. The interleaved intrinsic muscle bundles and fat are difficult to discern on CT and are best seen on T2-weighted (T2W) MR images.
• Floor of mouth
Floor of mouth (FOM) is a U-shaped space situated below the tongue. It is defined as the space between the mucosal surface and the mylohyoid (MH) muscle sling and comprising both the structures. The mylohyoid sling separates the floor of the mouth from the right and left submandibular space (SMS) and the midline submental space. Three important components of the floor of mouth are the following:
• The mylohyoid sling is formed by the right and left mylohyoid muscles. Each muscle arises from the mylohyoid ridge on the inner surface of the mandible from the symphysis to the last molar and extends posteriorly to attach to the hyoid. Medially, both the muscles insert into a fibrous median raphe. Two other muscles, the geniohyoid and the anterior belly of digastric, support the FOM. The muscles of the floor of the mouth are summarized in Table 3.8.2.
• The sublingual space (SLS) is located below the tongue, superomedial to the MH muscle, separated from the SMS that lies inferolateral to the MH muscle. These spaces contain glandular and fatty tissue that is easy to distinguish from the muscles both on CT and MRI. The SMS is not a part of the floor of the mouth as the caudal limit of the oral cavity is the MH sling. The contents of the SLS and SMS are enumerated in Boxes 3.8.2 and 3.8.3. The mylohyoid sling is deficient posteriorly allowing communication between the SLS and the SMS.
• The root of tongue consists of the lingual septum and the genioglossus and geniohyoid muscles. It is bound inferiorly by the MH muscle, anteriorly by the mandibular symphysis and along with the laterally positioned sublingual space that forms the floor of the mouth.
Arises from the mylohyoid ridge along the inner surface of mandibular body from symphysis to last molar tooth
The muscles of both the sides insert into the midline raphe and posteriorly attach to the hyoid bone
MH muscles of both sides come together to form the MH sling which is the inferior border of oral cavity
MH muscle of each side separates the superomedial sublingual (SLS) from the inferolateral submandibular (SMS). The muscle is deficient posteriorly allowing communication of the SLS and SMS.
MH muscle may sometimes have a defect called a “bouttoniere”, a potential communicating pathway between the SLS and the SMS.
Anterior belly of digastric (AG)
Arises from the digastric fossa on inner side of lower border of mandible.
Each muscle inserts on to the body and greater cornu of the hyoid bone.
These muscles lie below the MH in paramedian location within the SMS and are seen best on axial and coronal images.
AG muscle of each side forms a support for the MH muscle sling
Fat-filled region between the AG of both the sides is the submental space.
Geniohyoid (GH)
Arises from the inferior genial tubercle of mandible.
Inserts on the body of hyoid bone
GH and the GG muscles along with the midline lingual septum make up the root of tongue.
The anatomy of the FOM is best understood on axial and coronal images. Coronal images show the depth of the FOM, the entire extent of the MH sling and its relationship to the submandibular space. At CT, the various muscles of the floor of mouth cannot be differentiated based on their attenuation, and the anatomy of the FOM is best seen on MRI.
• Hard palate
The hard palate extends from the posterior aspect of the upper alveolar ridge to the soft palate and serves as the roof of the mouth separating the oral and nasal cavities. The bony portion of the hard palate is composed of the palatine process of the maxilla and the horizontal plate of the palatine bone and is covered by tightly adherent periosteum and mucosa. Important foramina in the palate are the following:
1. The incisive foramen is located immediately posterior to the maxillary incisors. It transmits the nasopalatine nerve that is a branch of the maxillary division of the trigeminal nerve (V2) from the floor of the nasal cavity as well as the nasopalatine artery, a branch of the sphenopalatine artery, supplying the oral mucosa covering the hard palate.
2. The greater and lesser palatine foramina are located at the posterolateral aspect of the hard palate directly anterior to the junction of the hard and soft palate; these foramina transmit the greater and lesser palatine vessels and nerves that are branches of the second division of V2.
Imaging options
1. Plain radiography
Plain radiographs are limited in their ability to detect osteolysis if bone loss is less than 12.5% and 6.6% for cortical and mineralized bone, respectively, and are unable to assess any associated soft-tissue abnormalities. Plain radiography has a limited role in radiological workup of patients with diseases of the oral cavities. Sialography may be used to evaluate obstructive sialadenitis and can demonstrate obstructive calculi and strictures.
2. Ultrasonography (USG)
USG is a readily available, inexpensive, fast, noninvasive imaging modality without the use of ionizing radiation. USG of the oral cavity and tongue is performed using intraoral and extraoral techniques with high-frequency (7–12 MHz) transducers. It can be used for evaluation of tumour thickness in oral cavity cancers and to assess salivary duct or gland diseases. However, being highly operator dependent, it may result in interpretation errors in hands with limited expertise.
3. Computed tomography (CT)
Contrast-enhanced multidetector CT scan (MDCT) provides faster acquisition coupled with excellent quality images and multiplanar reformations (MPRs) that in turn allow better assessment of cortical bone, any calcifications and nature and extent of the soft-tissue abnormality. Acquisition is done with the patient in supine position and the neck slightly hyperextended. To avoid dental amalgam artefacts, a second acquisition along the body of mandible (open mouth acquisition or gantry tilt) may be done. About 75–100 mL of iodinated CT contrast is used in adult population. All images are reviewed with soft tissue and bone algorithms. Puffed-cheek CT technique is particularly valuable in assessment of mucosa-based tumours of the oral cavity. In this technique, the patient blows uniformly through pursed lips while breathing normally. This allows air to separate the mucosal surfaces and thus helps differentiate whether a lesion is arising from the buccal or gingival mucosal surface.
4. Magnetic resonance imaging (MRI)
Only gold members can continue reading. Log In or Register to continue