Osseous Metastases
Skeletal metastases are the most common variety of bone tumors, particularly in the elderly patients. Some malignant tumors demonstrate a far greater predilection for osseous involvement than do others. Cancers of the breast, prostate, lung, and kidney account for about 80% of all metastatic lesions to bone. In men, carcinoma of the prostate accounts for about 60% and carcinoma of the lung for about 25% of all bone metastases. In women, carcinoma of the breast is responsible for about 70% of all metastatic lesions, the remaining 30% being mainly due to carcinoma of the thyroid, uterus, and kidneys. Other primary tumors responsible for bone metastases include carcinomas of the stomach, colon, urinary bladder, melanoma, and some neurogenic tumors. Some sarcomas, such as osteosarcoma and Ewing sarcoma, may also occasionally metastasize to the osseous structures. In children aged 5 years and younger, neuroblastoma is usually the primary tumor responsible for metastatic disease.
Metastases can be solitary or multiple, and they can be further subdivided into purely lytic, purely sclerotic, or mixed lesions. Osteolytic metastases are the most common, representing about 75% of all metastatic lesions. The primary source is usually a carcinoma of the kidney, lung, breast, gastrointestinal tract, and thyroid (Fig. 9.1). Osteoblastic metastases represent approximately 15% of all metastatic lesions. In men, they are caused mainly by primary carcinoma of the prostate or a seminoma. In women, the primary source is usually carcinoma of the breast, uterus, or ovary. In both genders, sclerotic metastases may originate from carcinoid tumors, urinary bladder tumors (particularly transitional cell carcinoma), certain neurogenic tumors (such as medulloblastoma), and osteosarcoma (Fig. 9.2). Mixed metastases (osteoblastic and osteolytic) represent approximately 10% of all metastatic lesions. Any primary tumor may give rise to mixed metastases, the most common primaries being breast and lung carcinomas. Cortical metastases are very rare, the primary tumor being almost invariably in the lungs. Acrometastases (metastatic lesions affecting the distal phalanges) are extremely unusual, and if present, the primary tumor is usually in the lung and less likely in the breast or kidney.
Histopathologically metastatic carcinomas are sometimes easier to diagnose than are some primary bone tumors because of their epithelial pattern. Occasionally, a metastatic lesion may exhibit a characteristic morphologic pattern that strongly suggests a source of primary tumor, such as the clear cells of hypernephroma, follicular or giant cell carcinoma of the thyroid, or the pigment production of melanoma. Moreover, some neoplasms are associated with the production of enzymes or antigens, which can be detected after the decalcification procedure. It is possible, for example, to perform a prostate-specific antigen (PSA) study or a prostate-specific acid phosphatase by immunohistochemistry to identify the primary tumor site in the prostate. The other studies may demonstrate nuclear transcription factors such as homeobox gene CDX2 (occurring in gastrointestinal carcinomas) or thyroid transcription termination factor I, TTFI (occurring in lung and thyroid cancers), or to analyze the pattern of cytokeratin (CK) filaments (e.g., presence of CK20 and absence of CK7 in GI but not in lung cancers), supplemented by additional immunoreactions of cytokeratins, classification determinant (CD) endothelial markers CD20, CD99, and neuron-specific enolase (NSE) for the differentiation of small round blue cell tumors, all leading to identification of unknown primary tumor.
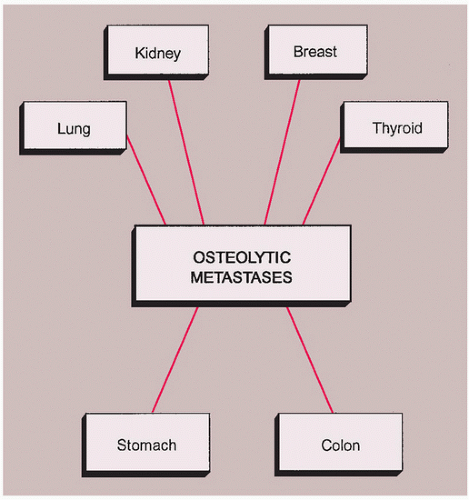 FIGURE 9.1 Origin of osteolytic metastases. |
SKELETAL METASTASES
Definition:
The spread of the cancer cells from the initial site of the tumor to the bones.
Epidemiology:
Metastases are relatively rare in patients younger than 40 years, most common after the sixth decade.
Both genders are equally affected.
Sites of Involvement:
Axial skeleton (skull, spine, pelvis).
Proximal segments of the limb bones.
Extremely rare distal to the elbows and distal to the knees.
Clinical Findings:
The majority of metastases are asymptomatic, at least in the early stages.
In advanced cases, pain is the primary symptom, rarely a pathologic fracture.
Imaging:
Radiographic features of skeletal metastases generally are not specific; solitary metastatic lesion may look just like a primary bone tumor (Figs. 9.3, 9.4, 9.5 and 9.6); however, periosteal reaction and soft-tissue mass are uncommon. Bubbly, highly expansive (blow-out) metastatic lesions usually originate from a primary carcinoma of the kidney or thyroid (Fig. 9.7). Metastases located in the cortical bone (so-called “cookie bite” or “cookie cutter” lesions) are characteristic for primary bronchogenic carcinoma (Figs. 9.8 and 9.9). Multicentric osteoblastic metastases in form of round sclerotic foci or diffuse increase in bone density are often seen in primary carcinoma of the prostate gland (Fig. 9.10A,B) or the breast (Fig. 9.10C). Multifocal osteolytic or even mixed metastases may look like multiple myeloma (Fig. 9.11).
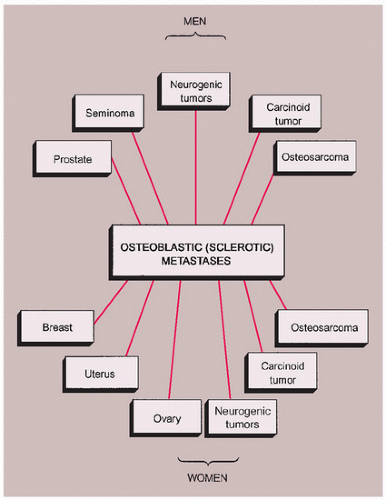
FIGURE 9.2 Origin of osteoblastic metastases.
Scintigraphy is the most sensitive modality to detect metastatic lesions in the skeletal system (Figs. 9.12 and 9.13). In addition, it is an effective modality in differentiating multifocal osteolytic metastases (almost invariably exhibiting positive findings on radionuclide bone scan in form of increased uptake of the radiotracer) from multiple myeloma (which usually displays a normal bone scan).
PET and PET-CT are very sensitive in demonstrating all metastatic lesions (Figs. 9.14, 9.15 and 9.16).
Magnetic resonance imaging shows variety of signal intensity, depending whether the metastasis is lytic, sclerotic, or mixed (Figs. 9.17 and 9.18). Occasionally, this modality is useful in determining the origin of the metastatic lesion, such as a “flow-void” sign apparently characteristic for metastatic renal carcinoma. Postcontrast studies show significant enhancement of highly vascularized metastatic lesions.
Pathology:
Gross (Macroscopy):
 FIGURE 9.3 Radiography of osteolytic metastasis. A 45-year-old man presented with a solitary osteolytic lesion in the left proximal tibia, originally misinterpreted as a giant cell tumor. An extensive clinical workup and excision biopsy lead to the diagnosis of metastasis from renal cell carcinoma. |
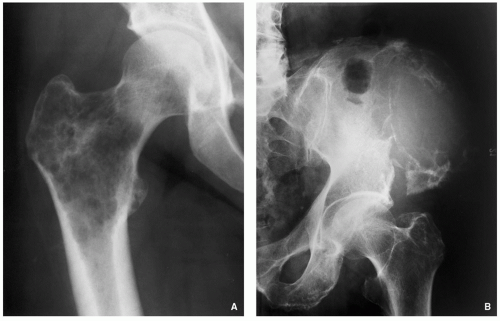 FIGURE 9.4 Radiography of osteolytic metastasis. (A) Anteroposterior radiograph of the right hip of a 52-year-old woman shows a large lytic lesion in the intertrochanteric region of the femur, proved to be a metastasis from carcinoma of the colon. (B) Anteroposterior radiograph of the left hemipelvis of an 83-year-old man shows an osteolytic lesion in the ilium, proved to be a metastasis from the thyroid carcinoma. |
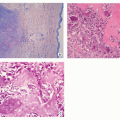
Histopathology:
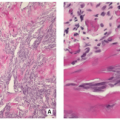
Many metastatic lesions exhibit a desmoplastic fibrotic reaction and the presence of woven or mature bone trabeculae with intertrabecular fibrosis (Figs. 9.19, 9.20 and 9.21).
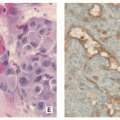
Poorly differentiated epithelial carcinoma cells or glandforming adenocarcinoma may indicate primary carcinoma in the colon (Fig. 9.22).
Metastatic melanoma may show variety of morphologic features with prominent pleomorphism and atypia. Identification of melanin pigment within the tumor cells is also a helpful diagnostic feature (Fig. 9.23).
Metastatic follicular carcinoma from the thyroid resembles the normal microscopic pattern of the thyroid gland. Foci of papillary formation and follicular elements with cells containing clear nuclei with pseudoinclusions may be present.
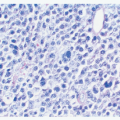
Presence of glycoproteins such as gross cystic disease fluid protein (GCDFP15) in the cells from metastatic breast carcinoma is a helpful diagnostic feature.
Metastasis from renal cell carcinoma may show clear cells.
Metastatic sarcomas show poorly differentiated spindle cells with prominent pleomorphism.
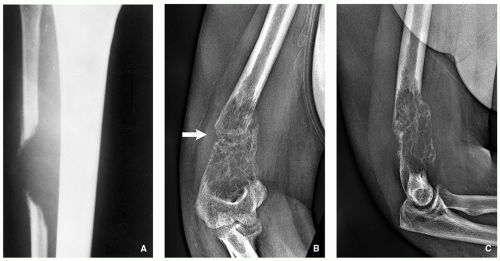 FIGURE 9.5 Radiography of osteolytic metastasis. (A) Anteroposterior radiograph of the right leg of a 41-year-old woman with renal cell carcinoma shows a lytic lesion in the fibula, breaking through the cortex and extending into the soft tissues. (B) Anteroposterior and (C) lateral radiographs of the right elbow of a 44-year-old woman with soft-tissue leiomyosarcoma of the buttock show lytic metastasis to the distal humerus. Note associated pathologic fracture (arrow). |
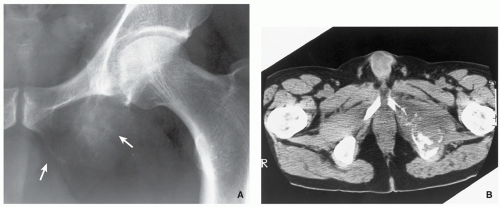 FIGURE 9.6 Radiography and computed tomography of osteolytic metastasis. (A) Anteroposterior radiograph of the left hip of a 50-year-old man with renal cell carcinoma shows an osteolytic lesion almost completely destroying the ischium (arrows). (B) Axial CT section demonstrates the extent of bone destruction and a soft-tissue extension. |
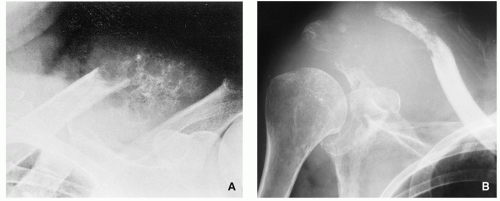 FIGURE 9.7 Radiography of osteolytic metastases. (A) Blown-out osteolytic metastasis in the acromial end of the left clavicle of a 52-year-old man with renal cell carcinoma (hypernephroma). (B) Blown-out osteolytic metastases in the acromial end of the right clavicle, acromion, and glenoid, associated with a soft-tissue mass of a 59-year-old woman with renal cell carcinoma. |
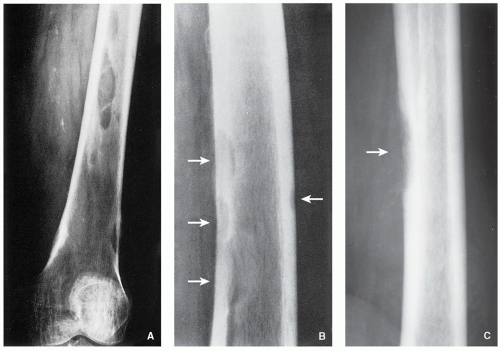 FIGURE 9.8 Radiography of cortical metastases. (A) Anteroposterior and (B) lateral radiographs of the left femur of an 82-year-old man with bronchogenic carcinoma show characteristic cookie bite appearance of the lesion (arrows). (C) Osteolytic cortical metastasis to the femur (arrow) of a 62-year-old man with bronchogenic carcinoma. |
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


