Fig. 26.1
Normal coronary arteries in 320-row CT in a patient with atrial fibrillation. Panel A shows the three-dimensional reconstruction and the ECG strip with atrial fibrillation (arrows in the inset). Panels B–D show curved multiplanar reformations along the left anterior descending, right, and left circumflex coronary artery, respectively, without significant diameter reduction. There is a small artifact in the mid-RCA, but otherwise image quality is very good. Images were acquired during one heartbeat with arrhythmia control using volume CT covering the entire heart in a single gantry rotation
Despite cost issues, it is, therefore, likely that the concepts of wide-area detector and multisource CT will eventually be merged within a single CT scanner, making the advantages of both approaches available for patient care. This may allow solving one of the most important issues in cardiac CT – limited temporal resolution.
26.1.2 Better Temporal Resolution
Further reducing the gantry rotation time (to below the currently achieved 270–350 ms) is an obvious approach to improving temporal resolution and reducing heart rate dependency. However, our ability to shorten the rotation time is limited by the dramatic increase in centrifugal forces that occurs as the rotation time is reduced. For instance, at a 400-ms rotation time, the relative centrifugal force is 18–20 g, which already requires considerable centripetal force to counteract. However, at 200 ms (equal to an image acquisition window of 100 ms with halfscan reconstruction), the relative centrifugal forces rise to 74–80 g because they are equal to the square of the velocity. New technologies such as an air-bearing CT gantry and faster data transfer systems might alleviate this problem and make it feasible to reduce the rotation time to 200 ms or even shorter. However, it is not very likely that a reduction in the rotation time alone will be pursued as a strategy for further improving temporal resolution. Instead, it is much more likely that the three concepts of (1) multisource scanning, (2) adaptive multisegment reconstruction and novel intelligent algorithms for improving temporal resolution by reconstruction methods, and (3) shortening the gantry rotation time will be developed further and combined in some fashion to improve temporal resolution.
26.1.3 Better Spatial Resolution
The current slice collimation of coronary CT angiography (between 0.5 and 0.75 mm) limits its application to small structures such as coronary plaque and its internal makeup. Thus, thinner slice collimation (e.g., of 0.2–0.3 mm) or better in-plane resolution (Chap. 9c) have the potential to improve the assessment of plaques and stents and facilitate the quantification of stenoses by coronary CT angiography (Fig. 26.2). However, reducing the slice collimation by a factor of 2 requires the radiation exposure to be increased by a factor of 2 (if the same detector technology is used) to keep the image quality constant. Thus, improvements in spatial resolution are not easily achieved using the current technology, and further developments (e.g., detector material) are necessary for clinical applications if one does not wish to increase radiation exposure again.
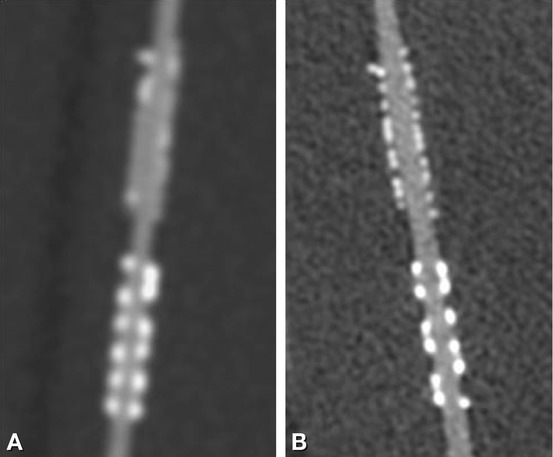
Fig. 26.2
Advantages of high-resolution (fine-cell detector) CT with a ~0.3-mm slice thickness for coronary stent imaging. Multiplanar reformations along a coronary stent with 2.5-mm inner diameter (in a phantom) obtained using 0.625-mm slice collimation and cell width (Panel A), and high-resolution CT with 0.3-mm slice collimation and cell width using a 0.3 × 0.3-mm focus size tube (Panel B). The opacified lumen within the small stent is more clearly seen, with fewer blooming artifacts, using the thinner slice collimation (Images courtesy of Sachio Kuribayashi. Department of Radiology, Keio University School of Medicine)
26.2 Clinical Developments
The expected upcoming clinical developments are summarized in List 26.2.
List 26.2. The foremost upcoming clinical developments
1.
Reliable coronary artery stent imaging
2.
Myocardial perfusion and viability imaging
3.
Imaging and follow-up of coronary plaques after medical interventions
4.
Application of CT to asymptomatic high-risk patients
26.2.1 Coronary Stent Imaging
The technical innovations described above may make possible the reliable assessment of coronary artery stents for the presence of restenoses. For this purpose, it will be instrumental to add the fourth dimension for myocardial CT perfusion imaging to our analysis and to reduce motion artifacts that are related to ECG irregularities or patients’ limited breath-hold capacity. Also, better spatially localized and temporally resolved quantitative measurements of the inner diameter of coronary stents will be pivotal to our efforts to broaden the clinical use of CT and extend it to the follow-up of patients who have undergone coronary stent placement.
26.2.2 Myocardial Perfusion and Viability Imaging
Another advantage of volume CT and second-generation dual-source CT is that a fourth dimension, time, can be added, making it possible to assess myocardial perfusion and coronary blood flow (Chap. 19




Related posts:




Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
