Chapter 26 Ovarian Cancer
Epidemiology
Ovarian carcinoma is a dismal disease, usually presents at an advanced stage, and remains the deadliest form of gynecologic malignancy. Ovarian cancer is the most common cause of death from cancer in women with gynecologic malignancy and results in 5% of overall deaths due to cancer.1 In the United States, an estimated 21,990 new cases and 15,460 deaths were projected for 2011.1
Ovarian cancer occurs sporadically in 90% of patients, and in only 10% of patients, it occurs with predisposing inherited syndromes.2 Various etiologies are connected to ovarian cancer, and the most important risk factor is a family history of the disease.3 These patients are usually younger, and most of them are premenopausal at presentation. Three different hereditary syndromes have been liked to these tumors. The most common of these is the breast-ovarian cancer syndrome, which has been linked to mutations in the BRCA1 and BRCA2 tumor suppressor genes.3,4 The lifetime risk of developing ovarian cancer in these women ranges from 15% to 30%, although some have reported it to be as high as 60%.4 Two other hereditary syndromes are the site-specific ovarian cancer syndrome and the nonpolyposis colorectal cancer or Lynch syndrome II. The Lynch syndrome is characterized by early-onset upper gastrointestinal tract cancer, colorectal carcinoma, upper urothelial tract cancer, endometrial cancer, and ovarian cancer.5
BRCA1 mutations have also been found in 8% to 10% of sporadic ovarian cancers,6 and these sporadic cancers occur in a predominantly older, postmenopausal population. One of the theories suggested is “incessant ovulation,” although its controversial.7–9 The hypothesis suggests that repeated minor trauma related to ovulation and repair predisposes the ovary to neoplasia. Several observations support this theory such as nulliparity, early menarche, and late menopause. Conversely, multiparity, late menarche, early menopause, and use of oral contraceptives (i.e., fewer ovulation cycles) reduce the risk.10 This theory can also describe the geographic differences in prevalence of ovarian cancer rates because ovarian cancer is seen more in industrialized countries, where women tend to have fewer children, and less in countries where birth rates are higher.11
Anatomy and Pathology
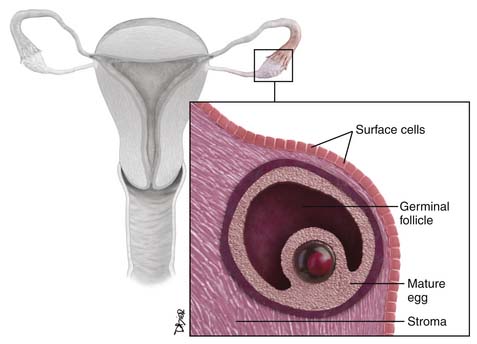
The ovaries are oval structures usually present in the pelvis and measure between 3 and 5 cm. The surface epithelial cells (Figure 26-1), which are derived from the coelomic epithelium, form a lining around them. The internal structure of the ovary is made of dense, fibrous tissue also called the stroma and is derived from the mesenchymal cells. The oocytes, which are also known as the germ cells, are located along the periphery of the stroma. The germinal cells form the follicles; these are surrounded by specialized cells of the mesonephric origin called the granulosa cells. The cells of the stroma immediately surrounding the follicles transforms to cells known as theca cells. The hilus cells of the ovary are similar to the testicular cells, known as Leydig cells, and produce hormones. There is a network of cellular cords and tubes, which is similar to a testicular structure known as the rete testis, and is called the rete ovary.12
Classification
The classification of ovarian tumors is developed by the World Health Organization (WHO) and the International Federation of Gynecology and Obstetrics (FIGO).13
Approximately 90% of primary ovarian cancers arise from the surface epithelium, which is similar to the mesothelium, which lines the peritoneal cavities and is also called the coelomic epithelium.12
The ovarian germ cell tumors arise from the germ cells of the ovaries.12
The sex cord tumors include tumors of mesonephric and mesenchymal origin. Fibromas and thecomas are fibrous in appearance, and some are derived from the granulosa cells or testicular sex cord counterparts, such as the Leydig and Sertoli cells.12
Surface Epithelial Tumors
Epithelial tumors account for approximately 60% of all ovarian tumors and approximately 90% of malignant ovarian tumors. The prevalence of these tumors usually increases with age and has a peak incidence between 60 and 70 years old. They are further divided into benign, borderline (low malignant potential), and malignant depending on their cellular proliferation.12,14 Based on their degree of differentiation, the malignant tumors can be categorized as well differentiated (10%), moderately differentiated (25%), and poorly differentiated (65%); the poorly differentiated tumors are associated with worse prognosis. The most common subtype of epithelial neoplasms is the serous tumors followed by mucinous neoplasms and endometrioid carcinomas. The clear cell carcinoma and the Brenner tumor are rare.15
Although sometimes difficult, the goal of radiologic assessment is to differentiate malignant tumors from benign tumors, rather than determining their histologic subtype. Sometimes, it may be possible to suggest the histologic subtype based on imaging features.16
Epidemiology and Pathology
Epithelial Tumors
Serous Tumors
Serous tumors are epithelial tumors and originate from the transformed cells of the coelomic epithelium, which resemble the internal lining of the fallopian tube. The benign serous tumors are usually unilocular but can be multilocular thin-walled cysts filled with watery straw-colored fluid.12 They usually do not have papillary projections, but if present, they are small compared with the borderline tumors. In up to 57% of patients, benign serous tumors are bilateral, occurring simultaneously in both ovaries.15 Most serous tumors are benign (60%), Fifteen percent are borderline and approximately 25% are malignant.
The malignant forms of these tumors tend to have a larger soft tissue component than the benign variety and can have focal areas of hemorrhage and necrosis.17 Microcalcifications (psammoma bodies) are seen in 30% of the malignant serous tumors at histologic analysis.18
Serous carcinomas are usually bilateral in more than 50% of cases.15 The primary neoplasm in these cases is small compared with the associated large-volume ascites. These tumors have large polypoid excrescences and may contain punctuate calcifications. Peritoneal carcinomatosis and omental caking are invariably seen in this setting.
Mucinous Tumors
Mucinous tumors are epithelial ovarian tumors that arise from the transformed cells of the coelomic epithelium that look like the cells of the endocervical epithelium (endocervical or müllerian type) or like the epithelium of the intestine (intestinal type).12
Benign mucinous tumors are usually multilocular with thin-walled locules filled with mucin, but they can be complicated with hemorrhage. One fourth of all benign ovarian neoplasms are mucinous tumors, and 75% to 85% of all mucinous ovarian tumors are benign.12 Benign mucinous tumors most frequently occur between the third and the fifth decades of life19 and are bilateral 21% of the time.15 Borderline mucinous tumors are similar to benign mucinous tumors but may have solid soft tissue nodules or papillar projections. The malignant counterparts have more solid components than the borderline tumors. Following rupture of these tumors, the endocervical mucinous tumors may be associated with mucinous tumorlets or implants whereas the intestinal type may be associated with pseudomyxoma peritonei. Most cases of pseudomyxoma peritonei arise from the appendiceal mucinous tumors with secondary involvement of the ovaries.12 Similarly 80% of mucinous tumors are benign, 10% to 15% are borderline and 5% to 10% are malignant.16
Endometrioid Tumor
These tumors are often malignant and may be cystic or predominantly solid.20 These are the second most common malignant ovarian surface epithelial tumors and occur in the sixth decade of life.19,20 Approximately 26% of these tumors are bilateral.15 Most malignant endometrioid tumors are confined to the ovaries and adjacent pelvic structures; 20% to 25% are associated with endometrial carcinoma.12 Malignant ovarian endometrioid carcinomas are considered to have a better prognosis than either mucinous or serous carcinomas.
Clear Cell Tumors
Clear cell tumors are epithelial ovarian tumors that are formed by clear, peglike or hobnail-like cells.12,21 These tumors are usually cystic and unilocular, containing solid rounded intramural nodules. Most clear cell tumors are malignant and represent 4% to 5% of all malignant ovarian epithelial tumors.12 They predominate in the fifth decade of life.19 Women with malignant clear cell tumors usually do not conceive, and approximately 50% to 70% of these tumors are associated with endometriosis.12
Transitional Cell Epithelial Tumors or “Brenner’s Tumors”
Transitional cell tumors arise from transformed cells of the coelomic epithelium that resemble transitional epithelium or the urothelium. These tumors are thought to be derived from surface ovarian epithelium that undergoes urothelium-like transformation (e.g., urothelial metaplasia, Walthard nests).22 They may be associated with similar tumors in the urinary bladder and are benign and consist of 1% to 3% of all ovarian tumors.23 They are solid and nodular, and most are unilateral. They can be found in conjunction with mucinous cystadenomas or other epithelial tumors.20 Most transitional ovarian tumors are very small, asymptomatic, incidentally discovered, and clinically irrelevant. They are usually seen in the fourth and fifth decades of life.23 Malignant transitional cell tumors can contain solid and cystic areas and intramural nodules.24 These tumors can associate with mucinous tumors in approximately 30% of cases that occur in the same ovary.16,25
Epithelial Tumors of Low Malignant Potential (Borderline Tumors)
Approximately 15% to 20% of all ovarian epithelial neoplasms are of borderline type and approximately 5% to 7% are mucinous type, the second most common type behind the serous borderline tumors.26 These are intermediate in their histologic and prognostic features between the benign cystadenomas and the clearly malignant carcinomas and lack stromal invasion. Compared with malignant serous tumors, borderline tumors are found in younger patients by 10 to 15 years. Malignant tumors are seen at approximately 45 years of age16,27 and account for one fourth of all ovarian neoplasms and two thirds of all ovarian serous tumors.12 The borderline tumors occur most commonly in childbearing age, show an indolent course, and usually have a better prognosis.28,29 They are usually seen in patients who are of childbearing age and approximately one third of the patients are nulliparous.28 The mucinous tumors are more common than the serous tumors.28 Serous tumors are frequently bilateral compared with the mucinous tumors. They are usually diagnosed during surgery and more than 90% of the tumors are stage I at presentation.28 Generally, these tumors present in a manner similar to other epithelial tumors and present with elevated CA125.28
Mixed Epithelial Tumors
Mixed epithelial tumors are composed of various subtypes of surface epithelial tumors. Every combination of epithelial tumors has been encountered. The tumor is named after the component that predominates but the tissue has to constitute greater than 10% of the entire tumor.20
Key Points Epithelial tumors
• Serous cystadenomas are cystic tumors that are often bilateral and unilocular and contain punctuate calcifications.
• Mucinous cystadenomas are cystic multilocular tumors with different consistencies of fluid and no solid component.
• Endometrioid tumors have solid and cystic components and are associated with hyperplasia or endometrial carcinoma.
• Clear cell cancers are usually benign and may be associated with endometriosis.
Germ Cell Tumors
Germ cell tumors arise from cells that are believed to be derived from primordial germ cells.12 Germ cell tumors usually occur in girls and adolescent females; the peak incidence is at 15 to 19 years30 and consists of 20% to 25% of all ovarian neoplasms20; only one third of these tumors are malignant.31,32 Conversely, most germ cell tumors occurring in adults are benign. Most tumors are large at presentation, and 85% of the patients present with abdominal pain mimicking appendicitis due to rupture, torsion, or hemorrhage; other symptoms include vaginal bleeding.33
Of all the germ cell tumors, the mature teratoma is benign and the rest are malignant. The malignant germ cell tumors are divided into dysgerminoma (the most common type) and nondysgerminomatous tumors. The most common types of nondysgerminomatous tumors are immature teratoma, yolk sac tumors, and mixed germ cell tumors. Less common variants of nondysgerminomatous tumors are embryonal carcinoma, polyembryoma, and nongestational choriocarcinoma.34
Benign Tumors
Mature teratomas are the most common germ cell tumors and are seen in the reproductive years.12 They are made of two or more mature embryonic germ cell layers. They are usually unilocular; in more than 80% of cases, they are filled with sebaceous material and lined by squamous epithelium.35 They have variable appearance depending on their contents such as hair follicles, skin glands, muscle, teeth, and other tissues. In rare cases, mature cystic teratomas may undergo malignant transformation, most often in postmenopausal patients, that most commonly results in squamous cell carcinoma.12
Malignant Tumors
Dysgerminoma
Dysgerminomas are rare and occur predominantly in young women. This tumor has a striking similarity to seminoma of the testis.36 Unilateral tumors are more common and 10% to 20% of dysgerminomas can be bilateral. They can be associated with congenital malformations of the genital tract and Turner’s syndrome. These tumors are usually solid and may contain cystic areas with hemorrhage and necrosis. Most occur in the second and third decades of life. Dysgerminomas account for 2% or less of all ovarian tumors and only 3% to 5% of all malignant ovarian tumors; nevertheless, they represent the most common type of malignant ovarian germ cell neoplasm occurring during pregnancy.12,20
Nondysgerminomas
Immature Teratomas
Immature teratomas represent less than 1% of all teratomas and contain primitive, immature, or embryonal structures in addition to well-developed or mature tissues.36,37 These tumors usually are unilateral, large, and predominantly solid; are rare; and occur in the first two decades of life.12 They have a solid soft tissue component, are invariably malignant, and grow rapidly. They rupture and disseminate via the lymphatic system and spread through the peritoneal cavity.
Endodermal Sinus Tumor (Yolk Sac Tumors)
Endodermal sinus tumor is a rare tumor, also known as yolk sac tumor, and displays cellular structures that resemble those of the primitive yolk sac. The tumor manifests as a large, complex pelvic mass that extends into the abdomen, contains both solid and cystic components, and tends to secrete alpha-fetoprotein.12
These tumors are malignant and usually occur in the second and third decades of life.36 Most of the tumors are usually unilateral and rare in postmenopausal women.12 No imaging features can distinguish them from other ovarian neoplasms.
Choriocarcinoma
Choriocarcinomas are germ cell tumors that arise from trophoblastic cellular elements.12 They typically are solid and have a hemorrhagic appearance. The majority of the primary ovarian choriocarcinomas are not related to pregnancy (nongestational). These occur in children and young adults. They secrete beta-human chorionic gonadotropin (β-hCG), which may lead to precocious puberty and abnormal uterine bleeding. Choriocarcinomas are highly malignant, have locally invasive spread mainly via lymphatics, and seed the peritoneal cavity.12
Key Points Germ cell tumors
• Germ cell tumors account for 15% to 20% of all tumors.
• Mature teratomas have calcifications in mural nodules and are benign; immature teratomas have scattered calcifications and are malignant.
• Yolk sac tumors are the second most common germ cell tumor and secrete alpha-fetoprotein.
• Choriocarcinomas are rare aggressive tumors that are widely metastatic at the time of presentation and secrete β-hCG.
Sex Cord–Stromal Tumors
Sex cord–stromal tumors are thought to originate from sex cords or the mesenchymal cells of the embryonic gonads. They account for approximately 8% of all ovarian tumors and affect all age groups. These tumors can be divided into two groups: one that develops from the gonadal stroma such as the fibromas, thecomas, sclerosing stromal tumors, and one that develops from the sex cord such as the granulosa cell tumors and Sertoli-Leydig tumors.38
Granulosa Cell Tumor
The adult granulosa cell tumors represent 95% of the sex cord tumors of the ovary, and they produce estrogen. These tumors occur commonly in peri- and postmenopausal women. The estrogen produced by the tumor can cause endometrial hyperplasia, polyps, or even carcinoma and is associated with these neoplasms in 5% to 25% of cases.12,38 The juvenile tumors can lead to precocious puberty. They account for 5% of all granulosa cell tumors.
Fibromas
Fibromas are benign tumors that arise from the spindle stromal cells that form collagen.12 They are usually seen in postmenopausal women and do not produce estrogen. They may be associated with nevoid basal cell carcinoma syndrome, also known as Gorlin’s syndrome.39
Sertoli-Leydig Cell Tumors
Sertoli-Leydig cell tumors are formed by cells that resemble epithelial and stromal testicular cells12 and occur in nulliparous women younger than 25 years.40 These tumors are rare, produce androgen, and in 30% of cases, can cause a virilization syndrome.38
Key Points Sex cord tumors
• Account for 5% to 10% of all tumors.
• Fibromas and fibrothecomas can mimic fibroids and can be associated with Meigs’ syndrome or Gorlin’s syndrome.
• Granulosa cell tumors are the most common tumors, are seen in postmenopausal women, and produce estrogen. They may cause postmenopausal bleeding and, if present in young females, cause precocious puberty.
• Sertoli-Leydig tumors are seen in females of reproductive age, produce testosterone, and can cause virilization
Metastatic Ovarian Tumors
Metastatic ovarian tumors account for approximately 15% of ovarian malignancies. The most common metastatic ovarian tumors seen are of gastrointestinal origin (39%), which is followed by breast (28%).41 Usually, these tumors are bilateral, large and can mimic primary ovarian neoplasms in 25% of cases.41 Depending on the geographic locations, the most common origin of these tumors can be colon or the stomach.41 These cancers are usually 5 to 10 cm in size and may have solid and cystic components.41
Patterns of Tumor Spread
In order to recognize the radiologic findings in each of the stages, it is important to thoroughly understand the mechanism of tumor spread. Ovarian carcinoma may spread directly to the surrounding pelvic tissues, such as the fallopian tubes, uterus, and contralateral adnexa, which are commonly involved, but direct extension of tumor to the rectum, bladder, and pelvic sidewall can also be seen.42 Tumor dissemination beyond the pelvis can occur via three mechanisms: intraperitoneal seeding, lymphatic invasion, and hematogenous dissemination.
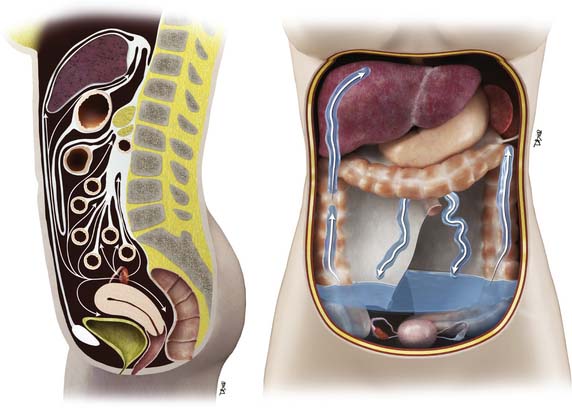
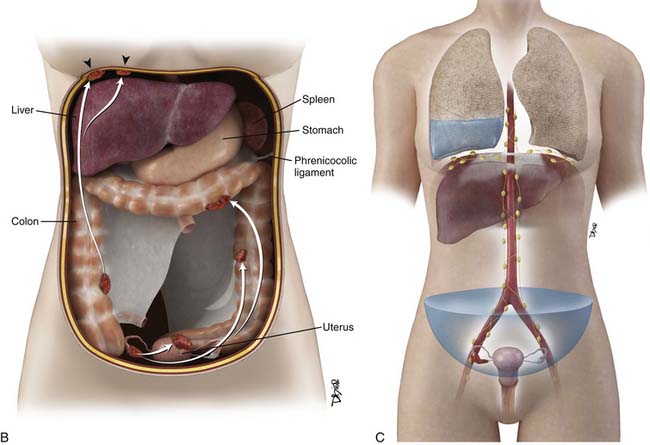
The most common mode of tumor spread in ovarian cancer is intraperitoneal dissemination (Figure 26-2), and approximately 70% of patients have peritoneal metastases at staging laparotomy. The greater omentum, right subphrenic region, and pouch of Douglas are the three most commonly involved sites found at laparotomy.43 Tumor deposits are uncommonly seen in the left subdiaphragmatic space because the inframesocolonic space is separated by the phrenicocolic ligament on the left. The malignant cells are shed from the tumor surface into the peritoneal cavity, and they follow the normal routes of peritoneal circulation. In the upright position, they will first fall into the cul-de-sac and other dependent portions of the pelvis; in the supine position, the fluid then flows into the paracolic gutters and eventually to the diaphragm.44 The fluid then flows more commonly to the right paracolic gutter, along the liver capsule, and the diaphragm.44 The peritoneal fluid then normally drains via the lymphatics of the diaphragm to the mediastinum via the internal mammary chain of lymph nodes.45,46 When these diaphragmatic lymphatics become occluded by tumor cells, the absorption of peritoneal fluid is impaired, resulting in accumulation of malignant ascites.
The lymphatic system also helps in dissemination of the ovarian cancer tumor cells. Lymphatic metastases can result from direct absorption by the lymphatic channels of the ovary versus absorption of tumor cells by the diaphragm.47 The ovaries have three pathways of lymphatic drainage. The main lymphatics follow the ovarian veins to the left para-aortic and the right paracaval lymph nodes at the level of the renal hilum and are the most common sites for metastatic adenopathy. The lymphatics of the broad ligament drain into the pelvic lymph nodes, external iliac, hypogastric, and obturator chain.18,45 Metastatic spread to the superficial and deep inguinal nodes can be seen when tumor spread occurs via the round ligaments.
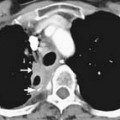
Hematogenous spread of disease is rare at presentation and has been reported in up to 50% of patients at autopsy.18,48 The most common sites of hematogenous involvement are the liver followed by the lung, but other locations including the brain, bone, adrenal gland, kidney, and spleen have all been reported.18,48,49 Although most tumors may spread in this fashion, serous and clear cell cancers predominantly spread via the lymph nodes.50,51 Some aggressive tumors such as choriocarcinomas and embryonal carcinomas commonly spread hematogenously.
Staging
The most common histologic types of ovarian cancer are serous, mucinous, endometrioid, clear cell, and undifferentiated tumors. These constitute 90% of ovarian cancers and arise from the surface epithelium.20 The overall prognosis is bad when these tumors become metastatic. However, the tumors of low malignant potential, formerly called “borderline tumors,” have a better prognosis. Histopathologically, they are usually either mucinous or serous tumors.14,52 Granulosa cell tumors, dysgerminomas, immature teratomas, endodermal sinus tumors, and metastases constitute the majority of the remaining malignant ovarian tumors.20,51 Approximately two thirds of patients have advanced disease at the time of diagnosis.53 Surgical exploration is typically performed to assign a disease stage based on the FIGO criteria, debulk the tumor, and confirm tumor histology.
There are two staging systems: the TNM (tumor-node-metastasis) system and the worldwide used, surgically based FIGO staging system.54 The FIGO staging system is shown in Table 26-1 and Figures 26-3 and 26-4. Accurate staging is performed with a staging laparotomy, which includes hysterectomy with bilateral salpingo-oophorectomy, pelvic and para-aortic lymph node biopsies, omentectomy, peritoneal biopsies, and washings.42,55 Tumor stage is a major prognostic factor.52 The overall 5-year survival rate depends on the tumor stage at presentation.53 The 5-year survival rate in descending order is 80% for stage I disease, 50% for stage II, 30% for stage III, and 8% for stage IV disease.14 Several other factors can affect prognosis such as histologic type, tumor grade, amount of residual disease after the initial cytoreductive surgery (debulking), and patient characteristics (age and performance status).52
Table 26-1 The Current FIGO Staging of Primary Ovarian Cancer, Proposed Changes and Classification(s) by the GCIG
| CURRENT FIGO STAGING | CURRENT FIGO CLASSIFICATION |
|---|---|
| Stage I | Growth limited to the ovaries |
| Stage IA | Growth limited to one ovary; no ascites present containing malignant cells. No tumor on the external surfaces; capsules intact |
| Stage IB | Growth limited to both ovaries; no ascites present containing malignant cells. No tumor on the external surfaces; capsules intact |
| Stage IC | Tumor either stage IA or IB, but with tumor on surface of one or both ovaries; or with capsule(s) ruptured; or with ascites present containing malignant cells or with positive peritoneal washings |
| Stage II | Growth involving one or both ovaries with pelvic extension |
| Stage IIA | Extension and/or metastases to the uterus and/or tubes |
| Stage IIB | Extension to other pelvic tissues |
| Stage IIC | Tumor either stage IIA or IB, but with tumor on surface of one or both ovaries; or with capsule(s) ruptured; or with ascites present containing malignant cells or with positive peritoneal washings |
| Stage III | Tumor involving one or both ovaries with histologically confirmed peritoneal implants outside the pelvis and/or positive retroperitoneal or inguinal nodes. Superficial liver metastases equals stage III. Tumor is limited to the true pelvis, but with histologically proven malignant extension to small bowel or omentum |
| Stage IIIA | Tumor grossly limited to the true pelvis, with negative nodes, but with histologically confimed microscopic seeding of abdominal peritoneal surfaces, or histologically proven extension to small bowel or mesentery |
| Stage IV | Growth involving one or both ovaries with distant metastases. If pleural effusion is present, there must be positive cytology to allot a case to stage IV. Parenchymal liver metastasis equals stage IV |
From Lerner JP, Timor-Tritsch IE, Federman A, Abramovich G. Transvaginal ultrasonographic characterization of ovarian masses with an improved, weighted scoring system. Am J Obstet Gynecol. 1994;170:81-85.

Patients can be understaged if a complete staging laparotomy is not performed. In more than 30% of patients, ovarian cancer is understaged at initial laparotomy; and in 77% of these cases, the tumor is presumed to be localized to the pelvis but subsequently is found to be stage III when a full staging procedure is performed.56 Incorrect staging may result in erroneous counseling about treatment options and prognosis. Sites of unsuspected disease most often include the pelvic peritoneum and tissues, ascitic fluid, para-aortic nodes, and diaphragm.57
Stage II
In stage II disease, there is local extension of tumor to involve the surrounding organs. In this stage, the tumor is confined to the pelvis without upper abdominal involvement. Stage IIA disease is characterized by either direct extension of tumor to the uterus or presence of implants on the uterus or the fallopian tubes. In stage IIB disease, tumor extends to involve surrounding pelvic tissues, rectum, bladder, and peritoneum. Imaging findings that suggest local extension of tumor are loss of tissue planes between the tumor and the bladder or the colon, less than 3 mm of space between the tumor and the pelvic sidewall, and presence of displacement or encasement of iliac vessels.58 Owing to the superior soft tissue contrast resolution, direct invasion is better seen with magnetic resonance imaging (MRI) than with either computed tomography (CT) or US.58
Stage III
While interpreting images, one should look carefully for subtle peritoneal thickening, nodularity, or enhancement of the peritoneal surfaces, which is an indication of peritoneal carcinomatosis.59 Presence of ascites in ovarian cancer is suggestive of peritoneal disease and aids in lesion conspicuity.60,61 The most common site of peritoneal spread of tumor is the omentum.62 This involvement may be microscopic, not visible on imaging or on visual inspection during surgery; however, it can be detected on histopathology.63 A fine reticulonodular pattern may be seen on radiology initially but is often subtle. Later, as disease progresses, there is often marked thickening resulting in omental caking. In addition, other common sites of involvement should be carefully evaluated, such as the subphrenic space, mesentery, and paracolic gutters. Coronal re-formats are usually helpful in evaluating the subdiaphragmatic regions.62
The small bowel is most commonly involved, by either serosal implants or frank bowel wall invasion, which can lead to bowel obstruction.48 This is the most common cause of morbidity in patients and has been reported in approximately 50% of autopsy cases.48 On imaging, the involved bowel usually appears thickened with resultant narrowing of the lumen. In stage III disease, along with peritoneal disease retroperitoneal, adenopathy has been reported in 27% to 44% of patients.62,64,65
Stage IV
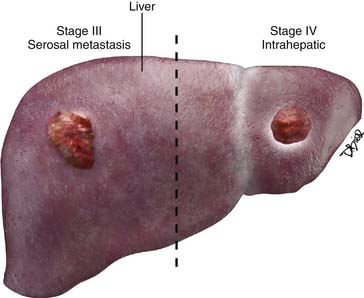
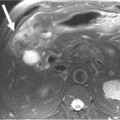
Stage IV disease is characterized by distant spread of tumor, which includes tumor spread to the pelvis and solid organs such as the liver. For a radiologist, it is important to differentiate implants on the liver capsule (stage III) from true parenchymal metastases (stage IV) because they are treated differently and have a different prognostic significance (see Figure 26-4




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


