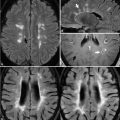
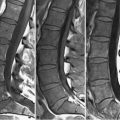
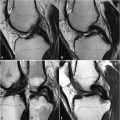
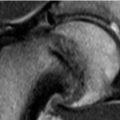
76 Ovarian Pathology Functional follicular ovarian cysts are common, benign entities, typically appearing as unilocular, thin-walled lesions with fluid-like SI (Fig. 76.1, axial T2WI). Nonfunctional cystic lesions are differential considerations, but because cystic neoplasia may appear similar, a newly diagnosed follicular cyst should be reassessed by ultrasound in 6 weeks. Walls of corpus luteum cysts are typically thicker, as illustrated in the coronal T2WI of Fig. 76.2A (white arrow), with the (B) contrast-enhanced T1WI demonstrating avid wall enhancement. Hemorrhagic corpus luteum cysts are common and are illustrated in Figs. 76.2C,D as high and low SI on axial (C, white arrow) T1 and (D) T2WI, respectively. Multiple bilateral cysts are seen in polycystic ovarian syndrome and ovarian hyperstimulation syndrome. Such cysts are small, peripheral, and subcapsular adjacent to prominent low SI central stroma. Accompanying ascites and pleural effusions are often seen in hyperstimulation syndrome. Teratomas may possess a cystic component. A dermoid (i.e., mature cystic teratoma) often contains prominent ectoderm, which secretes fatty sebaceous material. A solid nonenhancing protuberance (i.e., the Rokitansky or dermoid plug) containing fat, hair, bone, or teeth is often present. (A) T1WI in Fig. 76.3 illustrate a heterogeneously appearing cystic mass with prominent high SI components. Such hyper-intensity is seen in hemorrhagic cysts and endometriomas, but SI loss on (B
![]()
Stay updated, free articles. Join our Telegram channel



Full access? Get Clinical Tree


