Fig. 2.1
Coronal and sagittal views of 8.5 × 6.5 cm sacral chordoma involving S3-C1
2.4 Biopsy
Given that the differential diagnosis of sacral tumors is extensive, a biopsy should be performed in almost all cases. A transrectal or transvaginal biopsy should generally not be performed because it violates the containing membranes of presacral fascia and periosteum and could lead to seeding of the rectum or vagina with tumor cells. The preferred biopsy method is image-guided core biopsy, if it can be performed safely.
2.5 Benign Sacral Tumors
Most lesions of the sacrum are benign. Common benign sacral tumors in children are sacrococcygeal teratomas (the most common), lipomas, dermoids, epidermoid cysts, and bone islands or enostoses [18, 19]. Congenital abnormalities such as spina bifida occulta, tethered cord, hairy nevi, dermal sinus tracts, and dimples are associated with tumors of the sacrum in children [6, 20].
Sacrococcygeal teratomas are rare congenital tumors that arise from pluripotent cells. Although approximately 70% are benign, there is a tendency toward malignant transformation [18]. Approximately 20% of sacrococcygeal teratomas are identified prenatally; 70% are identified at birth, and the remaining 10% are identified within the first year of life. In adults, sacrococcygeal teratomas are rare and more commonly benign. On radiographs, the tumors are seen as protruding soft tissue masses with amorphous, punctuate, or spiculated calcifications. CT and MRI usually show a heterogeneous mixture of solid and cystic components [23]. Most sacrococcygeal teratoma resections are performed via a posterior approach, but occasionally a combined abdominal-sacral approach is required. In some patients, extent of resection warrants a temporary and rarely permanent colostomy [24].
While, in children, most sacral tumors tend to be benign, the frequency of benign lesions in adults is significantly lower. The most common benign sacral tumors in adults are giant cell tumors (13% of all sacral tumors), aneurysmal bone cysts, osteoblastomas, schwannomas, osteoid osteomas, skeletal osteochondromas, chondromyxoid fibromas, nerve sheath, and meningeal tumors of the sacrum [24–28, 58, 63].
The sacrum is the third most common location for giant cell tumors which tend to affect patients in their second and fourth decades of life. Giant cell tumors also tend to be more common in females [23, 28, 29]. Sacral giant cell tumors usually develop in an eccentric position, but commonly extend to involve both sides of the midline. Additionally, they tend to have the propensity to cross the sacroiliac joints and intervertebral disks, which is unusual for many other spinal lesions and is a useful distinguishing feature of giant cell tumors [23]. Although generally classified as a benign tumor, 5–10% of giant cell tumors have been reported to be malignant. Malignancy can be characterized based on mitotic activity, 1/mm2 or less is highly unlikely to be malignant, and histology and sarcomatous features within the primary specimen can indicate an increased likelihood of malignant degeneration. Additionally, patients may develop lung metastases and recurrence which demonstrate malignancy initially missed in primary tumor pathology evaluation. For these patients prognosis is poor and 5-year tumor-free survival is <50% [30]. The standard treatment for giant cell tumors is wide excision or aggressive curettage followed by adjuvant phenol, hydrogen peroxide, liquid nitrogen or argon beam therapy, embolization, and bone grafting or cementation. Cryosurgery and radiation therapy are also possible options [11, 30–34, 64]. It is important to attempt complete resection, as recurrence rates have been noted to be as high as 50% if complete resection is not achieved [10, 21, 35]. In appropriately selected patients, sacrectomy is an optional procedure which can render the patient free of disease and improve risk of recurrence [31, 32].
The second most common benign tumor in adults is an osteoblastoma. Typically, osteoblastomas affect young adults, with a male/female ratio of 2:1. Approximately 40% of these lesions occur in the spine with approximately 17% arising in the sacrum specifically [3]. Osteoblastomas should be excised. The lesions recur in 10–15% of cases, but the rate approaches 50% in the more aggressive pattern. Malignant transformation of osteoblastoma to osteosarcoma with metastases has also been reported [14].
There are additionally a handful of rarely occurring tumors of the sacrum, osteoid osteomas, cavernous hemangiomas, and chondromyxoid fibromas. Osteoid osteomas of the sacrum represent <2% of sacral tumors [4, 22, 58]. En bloc resection and radiofrequency ablation are both viable options and render low rates of recurrence [2, 33, 34]. Cavernous hemangiomas are the most common benign tumors of the spine, but only exceptionally involve the sacrum [36]. Chondromyxoid fibroma is a rare benign tumor of the sacrum [36]. Differential diagnosis should include chondrosarcoma, chordoma, and giant cell tumor. Surgical excision of the affected area or curettage and bone grafting are the treatments of choice for chondromyxoid fibroma. Radiation therapy should only be considered for the rare surgically inaccessible tumor [36]. Nonetheless, all of these lesions should be considered on the differential diagnosis when considering tumor subtypes.
Nerve sheath tumors may arise from the sacral nerve roots and include schwannomas and neurofibromas (Fig. 2.2). The most common nerve sheath benign sacral tumors are the giant sacral schwannomas; the mean diameter of these tumors is approximately 10.5 cm. Cyst formation, hemorrhage, and necrosis are relatively common in giant sacral schwannomas; unlike neurofibromas, schwannomas tend to be encapsulated. En bloc resection is the treatment of choice. Although difficult because of their size and the presence of critical sacral nerve roots, most can be resected completely, and recurrence is rare [37, 38].
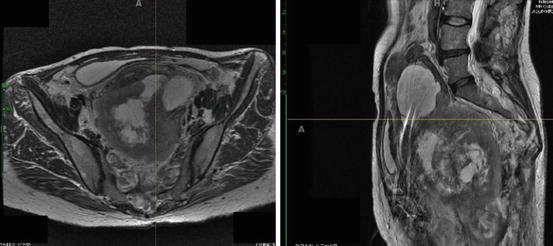
Fig. 2.2
Plexiform neurofibroma involving the sacrum in a patient with history of neurofibromatosis type 1
2.6 Malignant Sacral Tumors
The most common malignant tumors of the sacrum include chordomas, multiple myelomas, Ewing’s sarcomas, and primitive neuroectodermal tumors (PNET). Primary lymphomas, osteosarcomas, chondrosarcomas, angiosarcomas, fibrosarcomas, carcinoid, and amyloid tumors of the sacrum are also malignant, but are quite rare.
Chordomas are the most common primary malignant tumor of the sacrum and the most common tumor of any type involving the sacrum [29, 38]. The majority of sacral chordomas occur in the sacrococcygeal region in patients who are 40 years of age or older and occur almost twice as frequently in men compared to women [39]. Chordomas are slow growing and often displace but generally do not invade the rectum and/or the bladder (Figs. 2.3 and 2.4). Metastases are not common, and if metastatic disease is encountered, it is usually a late event [39]. On imaging, there is frequently a well-circumscribed osteolysis without an osteosclerotic rim, and a solid tumor with cystic areas is seen in approximately 50% of cases [3, 14, 15, 23]. Dedifferentiated chordoma is a rare variant that is clinicopathologically analogous to dedifferentiated chondrosarcoma. The sarcomatous component of dedifferentiated chordomas generally demonstrates more aggressive biological behavior and has a higher propensity to metastasize [40]. Primary treatment for chordomas is wide resection, and patient prognosis is dependent upon the completeness of resection and the violation of the tumor margins at the initial surgery. It is imperative to obtain an R0 resection to prevent recurrence; therefore, sacrifice of sacral nerve roots at the time of initial surgery may be necessary and is not uncommon. Total sacrectomy for chordomas involving the S1 nerve root have been reported [32, 41–43]. Local recurrence is the most important predictor of mortality in patients with chordomas and is related to the extent of initial resection. Local recurrence of sacral chordomas results in high morbidity rates and is associated with an approximately 20-fold increased risk of tumor-related death [8, 9, 11, 13, 39]. If the lesion is incompletely resected, adjuvant radiation therapy is another option; however, its efficacy is debatable [7, 11, 13, 44]. Results with brachytherapy techniques for recurrent sacral chordoma have been reported in small numbers of patients with varying success rates [45]. Chemotherapy has been of little value in the management of chordomas [11, 46]. Metastases, which can be found in the liver, lung, and regional lymph nodes, eventually develop in 5–43% of patients [44, 47].
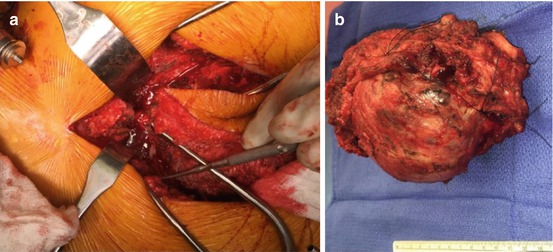
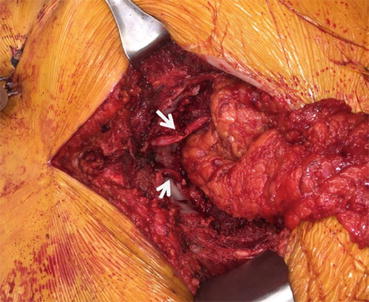
Fig. 2.3
(a) Prone approach to resection of sacral chordoma with attempted preservation of nerve roots. (b) Resected specimen
Fig. 2.4
Post-resection of chordoma with intact nerve roots (arrows)
Multiple myeloma is the second most common primary malignant neoplasm of the sacrum. Its incidence peaks in the sixth and seventh decade of life and is more common in males. The earlier solitary form, plasmacytoma, affects younger patients when compared with multiple myeloma. Lesions tend to be larger than those of multiple myeloma and tend to be osteolytic and expansile. These lesions also have poorly defined margins and are frequently associated with a soft tissue mass. Plasmacytomas generally progress to multiple myeloma in 10–15 years [14, 23, 48].
Lymphomas are the third most common primary malignant tumors of the sacrum but represent less than 5% of malignant bone tumors [30]. They predominantly affect men in their fifth to sixth decades of life. Lymphomas can cause aggressive bony destruction, although they tend to extend to the soft tissue leaving the underlying bones intact [14, 23, 49]. Three imaging signs, although nonspecific, are suggestive of lymphomas. These include the intensity and extent of uptake on bone scan (reveals a hot spot), the massive bone marrow invasion on MRI (poorly defined margins with a wide zone of transition) despite normal radiographic findings, and the large soft tissue mass with no visible cortical lesion on CT [50]. This highlights the importance of pursuing investigations (particularly bone scintigraphy and MRI) in patients with persistent pain despite their having no detectable abnormality on conventional radiography [15].
Ewing’s sarcoma and PNET represent the fourth most common primary malignant tumors of the spine [26, 61]. Within the spine, the sacrum is the most common site of involvement. The age range for Ewing’s sarcoma is 5–30 years, with 75% occurring in the first two decades of life. The male/female ratio is 3:1. Imaging findings tend to show paraspinal soft tissue masses and extradural space involvement [22, 51]. Some cases of sacral Ewing’s sarcomas may present as a predominant soft tissue mass, extending to pelvic structures or to the spinal canal, with limited osteolysis [15]. Immunohistochemical studies are needed to distinguish Ewing’s sarcoma from PNET, with the latter being characterized by neural differentiation [22, 23, 51, 60]. Primary treatment for Ewing’s sarcoma and PNET is chemotherapy and radiation therapy; however, many patients require decompressive surgery and stabilization secondary to symptomatology. Unfortunately, these lesions are associated with the worst prognosis when they occur in the sacrococcygeal region, with low likelihood of local control (60%) and poor long-term survival [19].
There are a number of more rare malignant sacral tumors. Osteosarcomas account for 4% of primary malignant tumors of the sacrum. Many of the osteosarcomas of the sacrum are secondary to Paget’s disease [30]. Sacral chondrosarcomas, fibrosarcomas, and angiosarcomas are unusual [52]. A 2% incidence of primary and secondary chondrosarcomas of the sacrum has been reported [4]. Most of sacral fibrosarcomas arise from a pre-existing lesion, usually previously irradiated bone, Paget’s disease, or fibrous dysplasia [3].
Another rare malignant lesion is a malignant peripheral nerve sheath tumors (MPNST) (neurofibrosarcomas or malignant schwannomas). These tumors are associated with neurofibromatosis type 1 as they usually arise from pre-existing neurofibromas. Additionally, they have a tendency to recur locally and spread hematogenously, and despite aggressive surgery and adjuvant therapy, the prognosis for patients with MPNST is poor [23].
2.7 Surgical Treatment of Sacral Tumors
For a majority of the aforementioned benign and malignant tumors, complete tumor resection with negative resection is the mainstay of therapy. The surgical goals should be to remove the tumor completely with clear margins while maximizing postoperative function. For malignant lesions, a radical surgical approach such as partial or total sacrectomy, with sacrifice of sacral roots, is often warranted to achieve total resection with clear margins [8]. Various sacrectomies have been described depending on the tumor location, extent, and histology, and decision regarding partial or total sacrectomy for en bloc resection can be made after radiological evaluation and appropriate tissue diagnosis.
Related posts:
 Osteoblastoma of the Sacrum
Tumors of the Sacrum: Diagnosis, Management, and Surgical Techniques
Anatomy and Surgical Approaches to the Sacrum
Osteoblastoma of the Sacrum
Tumors of the Sacrum: Diagnosis, Management, and Surgical Techniques
Anatomy and Surgical Approaches to the Sacrum
 Aneurysmal Bone Cyst of the Sacrum
Aneurysmal Bone Cyst of the Sacrum
 Soft Tissue Reconstruction Following Sacrectomy
Soft Tissue Reconstruction Following Sacrectomy
 Imaging of Sacral Tumors and Tumor Simulators: Experience of the Mayo Clinic
Imaging of Sacral Tumors and Tumor Simulators: Experience of the Mayo Clinic
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


