PACS Fundamentals
Objectives
On completion of this chapter, you should be able to:
• Define picture archiving and communication system (PACS).
• Compare and contrast the various types of PACS display workstations.
• Differentiate among the different types of digital imaging work flow.
• Define system architecture and recognize the three major models.
• Summarize the common functions found on a PACS workstation.
• Describe the situations and users that may require advanced PACS workstation functions.
Key Terms
Client/server-based system
Digital imaging and communications in medicine (DICOM)
Display workstation
Distributed or stand-alone system
File room workstation
Hanging protocol
Navigation functions
Picture archiving and communication system (PACS)
Quality control (QC) station
Reading station
Review workstation
Softcopy
Study
System architecture
Web-based system
Workflow
The picture archiving and communication system (PACS) is becoming more commonplace in today’s hospitals because hospital administrators have come to see the necessity of having such a system to serve physicians and patients even though it is expensive. The initial capital cost is great, but the benefit of having the system far outweighs the cost. This chapter outlines the basic concept of a PACS and its components, describes common PACS architecture, and gives examples of typical PACS work flows that may be seen in a hospital.
Fundamentals
As discussed in Chapter 1, a PACS consists of digital acquisition, display workstations, and storage devices interconnected through an intricate network (Figure 9-1). The PACS is an electronic version of the radiologist reading room and the file room. The first PACSs were used in the early 1980s and generally served a single modality. Large research institutions housed early systems because most were developed by the scientists who worked at those institutions. As vendors became more involved, they developed proprietary systems that were very specific to their modalities. Finally, as physicians and hospitals became interested, it was determined that there must be standardization.
Digital imaging and communications in medicine (DICOM) is a universally accepted standard for exchanging medical images among the modality, viewing stations, and the archive. First completed in 1985, this standard laid the groundwork for the future development of integrated PACSs. Now each modality and PACS communicates via DICOM, and DICOM continues to be refined every year. Every vendor and modality boasts DICOM compatibility (Figure 9-2), but each DICOM statement must be read carefully to determine the extent of the compatibility. DICOM compatibility issues are outside of the scope of this textbook.
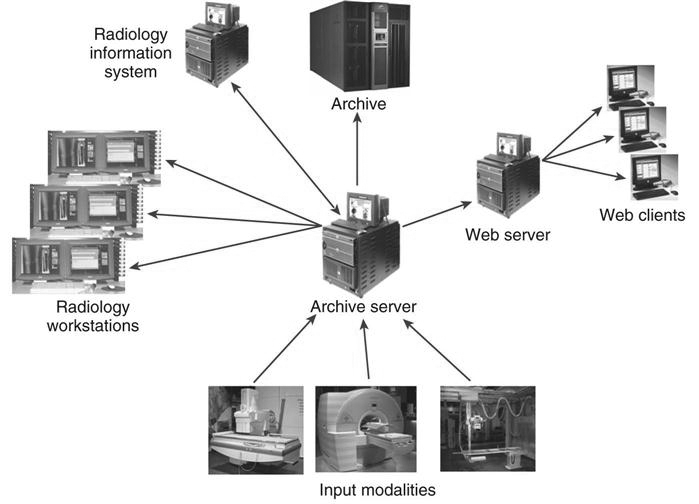
To understand what a PACS is and how it is used, it helps to look at the system’s individual parts. The following sections break down a PACS into its three fundamental parts (Figure 9-3): image acquisition, display workstations, and archive servers. Each of these topics is covered in depth in other chapters of the book.
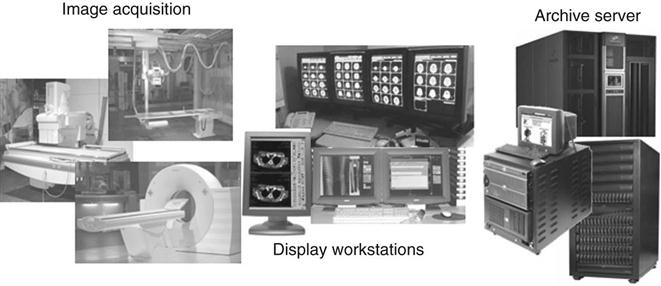
Image Acquisition
In modern radiology departments, most images are acquired in a digital format, meaning that the images are inherently digital and can be transferred via a computer network. Ultrasound, computed tomography (CT), magnetic resonance imaging (MRI), and nuclear medicine have been digital for many years and have been taking advantage of PACS far longer than general radiography has. As stated earlier, the first PACS served a single modality, namely, ultrasound. Ultrasound mini-PACS networks were the norm in many hospitals. Radiologists routinely made diagnoses by looking at images on the modality’s computer screen. It was a natural step from there to convert ultrasound to softcopy reporting (i.e., reading images on the computer without hardcopy films).
As the CT and MRI image sets became larger because of the increased number of cross-sectional images per patient, radiologists routinely went to the modality to view the images. This slowed down the scanning process for the technologists, and vendors began getting requests for extra console stations for radiologist viewing. These workstations were directly connected to the modalities. Radiologists could view the large stacks of images and perform simple image manipulation. These workstations morphed into mini-PACS and eventually into full-blown systems for CT and MRI. As discussed in Chapters 4 through 7, general radiography has taken the digital leap with digital projection radiography. Now the conversion to a completely digital radiology department is a reality.
Display Workstations
A display workstation is any computer that a health care worker uses to view a digital image (Figure 9-4). It is the most interactive part of a PACS, and these workstations are used inside and outside of radiology. The display station receives images from the archive or from the various radiology modalities and presents them for viewing. The display workstation has PACS application software that allows the user to perform minor image-manipulation techniques to optimize the image being viewed. Some display stations have advanced software to perform more complex image-manipulation techniques. More details about display workstations are given later in the chapter.

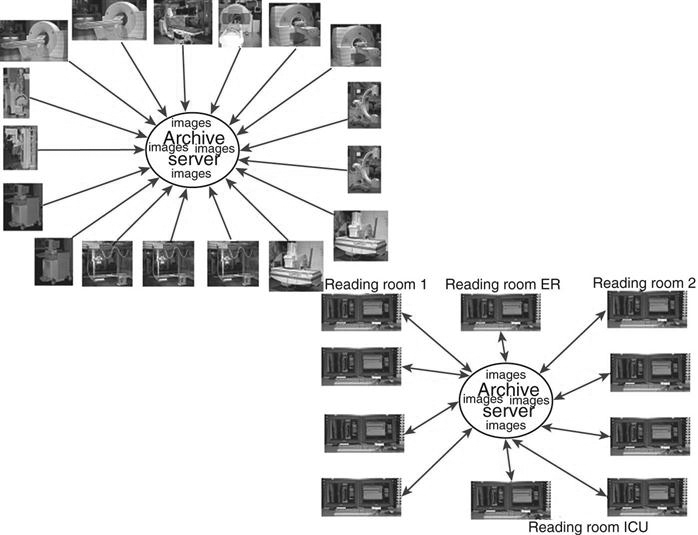
Archive Servers
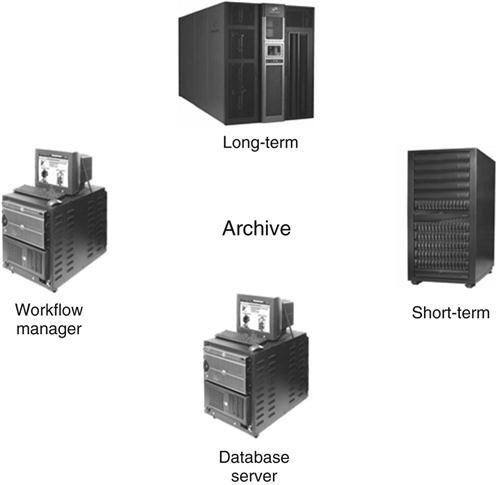
An archive server is the file room of the PACS. It is composed of a database server or image manager, short-term and long-term storage, and a computer that controls the PACS workflow, known as a workflow manager (Figure 9-5). The archive is the central part of the PACS and houses all of the historic data along with the current data being generated. In many institutions the archive serves as the central hub that receives all images before they are released to the radiologists for interpretation. The archive and all of its components are studied in depth in Chapter 10.
Workflow
Workflow is a term that can be used in any industry or in any organization. It simply means how a process is done, step by step. In radiology, the term workflow has always been used to describe how an examination is completed, from order entry to transcribed report. This section describes a generic film-based workflow and then compares it with a generic PACS workflow. The workflow in each radiology department is different because there are many variables.
Film-Based Workflow.
Most departments were designed years ago for film and chemical processing. Pass boxes were built into walls that fed into darkrooms and into large open reading rooms that had gigantic multiviewer lightboxes lining the walls (see Figure 9-11). Eventually chemical-processing time decreased from a few minutes to less than 60 seconds in some cases. As film and processing technology advanced, workflow became more efficient, despite the fact that technologists still have to hand-deliver film to radiologists and make the occasional copy for a referring physician.
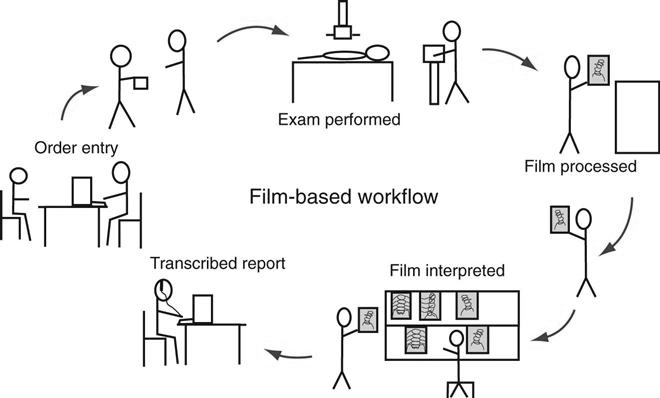
The following list outlines a typical workflow in a radiology department, from entering the order to transcribing the report (Figure 9-6).
• The first step in any radiology department workflow is the entry of the order. The order may be a paper prescription from the ordering doctor, or the order may have been placed in the computer system by any hospital staff member. Either way, an order is placed in the radiology information system (RIS), and a requisition is generated. A requisition generally contains the following information:
• Patient’s hospital identification (ID) number
• The paper requisition is then passed on to the technologist who will be performing the examination.
• The technologist prepares the room for the patient and brings the patient back to the room.
• The technologist critiques each film and repeats exposures as necessary.
• The technologist makes copies if necessary and releases the patient with the copies.
• The radiologist reads the films and dictates a report into the dictation system.
Generic PACS Workflow.
The PACS workflow is in many ways different from the film-based workflow (Figure 9-7). The technologist may get the order via an electronic worklist or a paper requisition, but after that, the process begins to change.
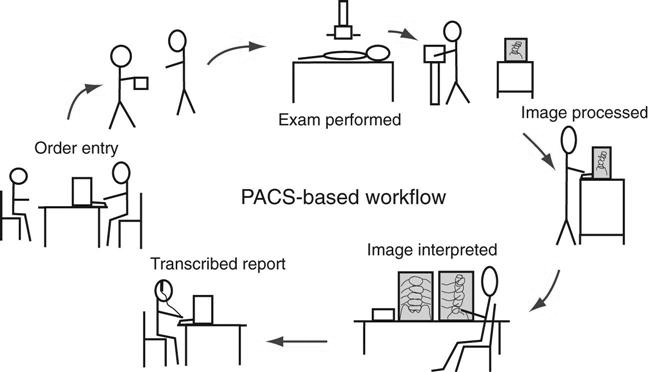
With PACS it is possible that the time it takes from performing the examination to completing the final radiologist’s report is only a couple of hours, compared with a couple of days for the film-based workflow.
System Architecture
System architecture can be defined as the hardware and software infrastructure of a computer system. In a PACS, the system architecture normally consists of acquisition devices, storage, display workstations, and an image management system. The following discussion outlines three common PACS architectures and takes a look at the flow of images after acquisition.
Client/Server-Based Systems
In a client/server-based system, images are sent directly to the archive server after acquisition and are centrally located (Figure 9-8). The display workstation functions as a client of the archive server and accesses images based on a centralized worklist that is generated at the archive server. The health care worker at the display workstation chooses a name from the central list, and the archive server sends the image data to the display station. After the “client” is finished, the image data are flushed from its memory. Most systems allow basic image manipulation at the display workstation or “client,” and the changes are saved on the archive server.