A. Ampullary stenosis
B. Chronic pancreatitis
C. Pancreatic ductal carcinoma
D. Duodenal carcinoma
2 Pancreatic neuroendocrine tumors are associated with which of the following syndromes?
A. Multiple endocrine neoplasia type 1
B. Multiple endocrine neoplasia type 2a
C. Multiple endocrine neoplasia type 2b
3 A patient presenting with epigastric pain is clinically suspected to have acute pancreatitis. What is the most sensitive and appropriate test in making the initial diagnosis?
A. CT
B. Serum insulin level
C. MRI
D. Serum lipase level
4a A 78-year-old man with bloating underwent a CT scan followed by an 111Indium-labeled octreotide scan. What is the most likely diagnosis of the finding at the pancreatic tail?

A. Pancreatic lymphoma
B. Pancreatic neuroendocrine tumor
C. Pancreatic ductal adenocarcinoma
D. Intrapancreatic splenule
4b What is the most common subtype of functioning pancreatic neuroendocrine tumor?
A. Gastrinoma
B. VIPoma
C. Insulinoma
D. Glucagonoma
5 A 42-year-old woman presents with abdominal pain and the CT shown below. What is the most likely cause of this diagnosis?

A. Hyperlipidemia
B. Gallstones
C. Heavy alcohol consumption
D. Cystic fibrosis
6 A 60-year-old man presents with left upper quadrant pain and weight loss. Based on the MR images shown, what is the most likely diagnosis?

Top row: FS T2W and FS T1W images. Bottom row: Arterial and venous phase FS T1W+gad.
A. Mucinous cystadenocarcinoma
B. Intraductal papillary mucinous neoplasm
C. Neuroendocrine neoplasm
D. Pancreatic ductal adenocarcinoma
7a Two days following an assault, this 31-year-old man developed abdominal pain and underwent CT. Which of the following is the most appropriate next step in management?

A. Serum amylase and lipase levels with serial abdominal examinations
B. Diagnostic peritoneal lavage with amylase level on collected fluid
C. Emergent reconstruction with Whipple procedure
D. Endoscopic retrograde cholangiopancreatography
7b Following surgical exploration and placement of surgical drains, the patient underwent an ERCP. What is the finding?

A. Acinarization of contrast
B. Pancreatic duct injury
C. Bile leak
D. Pseudoaneurysm
7c Which of the following is true regarding pancreatic injuries?
A. The most reliable method for determining injury severity is by measuring serum amylase level.
B. Ultrasound can readily differentiate pancreatic laceration from edematous pancreatitis but cannot reliably determine parenchymal depth of injury.
C. Pancreatic lacerations most often occur at the uncinate process due to compression against the spine.
D. Main pancreatic duct disruption usually requires surgery as stenting alone is rarely successful.
8 A 39-year-old man presents with symptoms of epigastric pain and vomiting. Based on the CT images shown below, what is the most likely diagnosis?

A. Intraductal papillary mucinous neoplasm
B. Groove pancreatitis
C. Ampullary carcinoma
D. Duodenal diverticulitis
For each patient in questions 9 to 15, select the most likely diagnosis (A to H). Each option may be used once, more than once, or not at all.
A. Intraductal papillary mucinous neoplasm
B. Serous microcystic cystadenoma
C. Mucinous cystic neoplasm
D. Solid pseudopapillary tumor
E. Cystic fibrosis
F. Mature teratoma
G. Choledococele
H. Duodenal diverticulum






15 31-year-old woman.

Top row: Contrast-enhanced CT and FS T2W MRI. Bottom row: Pre- and postcontrast FS T1W MRI.
16 A 57-year-old man presents with abdominal pain and weight loss. Based on the CT images below, the most appropriate treatment strategy is

Two axial and one coronal CT image from the late arterial phase.
A. Surgical resection
B. Chemotherapy and radiation
C. Percutaneous drainage catheter placement
D. Endoscopic pancreatic duct stent placement
17 A 60-year-old woman presents with abdominal pain. What abnormality is demonstrated on these axial and coronal CT images?

A. Annular pancreas
B. Ampullary carcinoma
C. Papillitis
D. Ectopic pancreatic rest
18 A 30-year-old woman presents with increase in abdominal pain. What is the diagnosis?


Coronal MIP and axial T2W images from MRCP.
A. Autoimmune pancreatitis
B. Chronic pancreatitis with ductal stone
C. Intraductal papillary mucinous neoplasm
D. Serous cystadenoma
19a A 39-year-old woman with diarrhea and abdominal discomfort was evaluated with CT and MRI. Based on the images shown below, which statement is TRUE regarding the appearance of the pancreatic head?

A. There is signal loss on the fat-saturated MR image compared to the non– fat-saturated image.
B. There is signal loss on the out-of-phase MR image compared to the in-phase image.
C. Enhancement on the venous phase MR image is greater than the arterial phase.
D. Enhancement on the arterial phase MR image is greater than the venous phase.
19b What is the diagnosis based on the images in the previous question?
A. Lipoma
B. Pancreatic ductal adenocarcinoma
C. Pancreatic neuroendocrine tumor
D. Focal fatty infiltration
20 For items 1 to 4, match the description of the pancreatic surgical procedure with the name (A to E). Each option may be used once or not at all.
A. Distal pancreatectomy
B. Central pancreatectomy
C. Whipple procedure
D. Beger procedure
E. Frey procedure
1. Resection of the pancreatic head and duodenum, followed by Roux-en-Y reconstruction.
2. Usually performed with splenectomy.
3. Excavation of the pancreatic head, followed by a longitudinal opening of the dilated pancreatic duct with a side-to-side pancreaticojejunal anastomosis.
4. Resection of a portion of the pancreatic neck or body, followed by pancreaticojejunostomy of the remnant tail.
21a A 60-year-old woman presents with abdominal pain. She is found to have an elevated lipase and amylase. Two images from a subsequent CT are shown. What is the diagnosis?

A. Interstitial edematous pancreatitis
B. Perforated duodenal ulcer
C. Necrotizing pancreatitis
D. Perforated jejunal diverticulitis
21b In what range is the CT severity index for the patient in the previous question?
A. 0 to 3
B. 4 to 6
C. 7 to 10
D. Unable to be determined on these images
21c The patient has a prolonged hospital course and is discharged. Twelve weeks after initial imaging, she has a repeat CT scan shown below. What is the appropriate term to describe the pancreatic finding?

A. Pseudocyst
B. Walled-off necrosis
C. Abscess
D. Acute necrotic collection
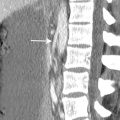
22 A 77-year-old woman patient has a distant history of a surgical procedure. What is the structure labeled with arrows on the CT?

A. Normal afferent limb
B. Recurrent cystic pancreatic neoplasm
C. Gallbladder
D. Abscess

A. Pancreas divisum
B. Chronic pancreatitis
C. Annular pancreas
D. Pancreatic ductal adenocarcinoma

A. Serous microcystic cystadenoma
B. Santorinicele
C. Side-branch intraductal papillary mucinous neoplasm
D. Duodenal diverticulum
24 Which hormone may be administered intravenously during MRCP to improve visualization of the pancreatic duct?
A. Cholecystokinin
B. Secretin
C. Glucagon
D. Insulin
25a What is the likely diagnosis on this abdominal CT?

Image courtesy of Dr. Priya Bhosale, Department of Diagnostic Radiology, The University of Texas, MD Anderson Cancer Center, Houston, Texas.
A. Acute necrotizing pancreatitis
B. Pancreatic metastasis
C. Pancreatic lymphoma
D. Autoimmune pancreatitis
25b Elevation of which serum marker is most specific for autoimmune pancreatitis?
A. IgG4
B. CRP
C. CA19-9
D. Chromogranin A
26 A 66-year-old man presented with persistent abdominal pain and weight loss 6 months after hospitalization for gallstone pancreatitis. Which statement is TRUE regarding collections in pancreatitis?

Axial CT image with contrast before intervention. Axial and scout CT images after intervention.
A. The majority of acute peripancreatic fluid collections require drainage.
B. The majority of infected collections can be identified on CT by the presence of gas.
C. Infection occurs more frequently in pseudocysts than walled-off necrosis.
D. CT guidance is preferred over ultrasound guidance during percutaneous drainage.
27 A 70-year-old man with a history of extrapancreatic malignancy underwent surveillance CT. Arterial and venous phase images are shown. Which of the following primary malignancy is the most likely etiology of this pancreatic mass?

A. Lymphoma
B. Melanoma
C. Renal cell carcinoma
D. Lung carcinoma
28a On day 4 of admission for acute pancreatitis, this patient experienced increasing abdominal pain and a CT scan was performed. The patient was hemodynamically stable. The most appropriate next step in management is:

A. Percutaneous drainage with catheter placement
B. Open surgery with debridement
C. Angiography with embolization
D. Treatment of symptoms with IV fluids and pain medication

A. Gastroduodenal artery
B. Proper hepatic artery
C. Inferior mesenteric artery
D. Superior mesenteric artery
ANSWERS AND EXPLANATIONS
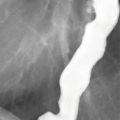
1 Answer C.Coronal image from MR cholangiopancreatography (MRCP) demonstrates dilation of the pancreatic and biliary ducts consistent with the “double-duct” sign. The most common cause is obstruction by pancreatic ductal adenocarcinoma. Other neoplasms of the ampulla, pancreas, and periampullary region such as duodenal carcinoma can also produce the double-duct sign. Benign causes include chronic pancreatitis and ampullary stenosis. Dilation of multiple side branches in addition to the main pancreatic duct, as seen in this case, may or may not be evident.
References: Ahualli J. The double duct sign. Radiology 2007;244(1):314–315.
Lopez Hänninen E, Amthauer H, Hosten N, et al. Prospective evaluation of pancreatic tumors: accuracy of MR imaging with MR cholangiopancreatography and MR angiography. Radiology 2002;224(1):34–41.
2 Answer A.The majority of pancreatic neuroendocrine tumors (NETs) are sporadic, but some are associated with genetic syndromes. About a quarter of tumors are found in patients with multiple endocrine neoplasia type 1 (MEN-1) and are the major cause of mortality. Patients with MEN-1 are predisposed to developing parathyroid adenomas or hyperplasia, pancreatic NETs, and pituitary adenoma (“pa, pa, pi”). Von Hippel-Lindau (VHL) disease is a rare hereditary syndrome with a broad spectrum of clinical features, and pancreatic findings in VHL include simple cysts, NET, serous microcystic cystadenomas, and rarely ductal adenocarcinomas. Two other syndromes, neurofibromatosis type 1 and tuberous sclerosis, have also been linked with pancreatic NETs. Pancreatic lesions are not a feature of MEN-2a or MEN-2b. MEN-2a is associated with medullary thyroid cancer, pheochromocytoma, and parathyroid adenomas (“me, phe, pt”). MEN-2b is associated with medullary thyroid cancer, pheochromocytoma, and neuromas (“me, phe, ne”).
References: Kim KW, Krajewski KM, Nishino M, et al. Update on the management of gastroenteropancreatic neuroendocrine tumors with emphasis on the role of imaging. AJR Am J Roentgenol 2013;201(4):811–824.
Scarsbrook AF, Thakker RV, Wass JA, et al. Multiple endocrine neoplasia: spectrum of radiologic appearances and discussion of a multitechnique imaging approach. Radiographics 2006;26(2):433–451.
3 Answer D.Most patients with acute pancreatitis (AP) can be diagnosed without imaging based on clinical presentation and elevated laboratory values. Serum lipase level is more sensitive than imaging in the diagnosis of acute pancreatitis. Serum insulin levels have no role in diagnosis of AP.
The role of imaging in the setting of uncomplicated AP is primarily to identify cholelithiasis as a treatable cause. Ultrasound is the most appropriate imaging study for this purpose. Cholelithiasis and heavy alcohol consumption together account for about 90% of cases of AP in developed countries. If the diagnosis of AP is equivocal or if worsening symptoms suggest a complication such as necrosis, contrast-enhanced CT scan would be appropriate. MRCP may be helpful in patients with suspected choledocholithiasis or pancreatic duct stone. MRI with contrast may have a secondary role in follow-up of complications of AP in patients with iodinated contrast allergy or young patients who require repeated imaging.
References: ACR Appropriateness Criteria: acute pancreatitis. American College of Radiology website. http://www.acr.org/~/media/ACR/Documents/AppCriteria/Diagnostic/AcutePancreatitis.pdf. Published 1998. Updated 2013. Accessed June 20, 2014.
Shinagare AB, Ip IK, Raja AS, et al. Use of CT and MRI in emergency department patients with acute pancreatitis. Abdom Imaging 2015;40(2):272–277.
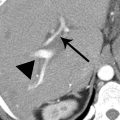
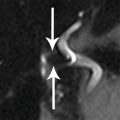
4a Answer B.There is a well-circumscribed mass in the tail of the pancreas on axial CT images, with enhancement greater on the arterial phase than venous phase. This pattern of enhancement indicates a hypervascular neoplasm and is compatible with a pancreatic neuroendocrine tumor (NET). The SPECT image from the 111In-octreotide scan shows uptake, confirming NET. (Not all NETs will show uptake, so a negative scan does not exclude NET.) Two additional cases of pancreatic NET are shown below. Large tumors are more likely to be heterogeneous with cystic, necrotic, or calcified components. The NET in the image on the left is heterogeneous and shows a calcification (arrowhead). About 15% of pancreatic NETs are cystic and difficult to differentiate from other cystic pancreatic lesions. A clue to a cystic or necrotic NET is a hypervascular rim (arrows) on the arterial phase image on the right.

A metastasis from renal cell carcinoma is also hypervascular and should be considered in the appropriate clinical setting. Splenules (accessory spleens) can be seen at the pancreatic tail and mimic a NET. Splenules should follow splenic enhancement on all phases. The arterial phase may demonstrate the serpiginous “arciform” or “moiré” sinusoidal enhancement diagnostic of splenic tissue. Splenules show uptake on 99mTc-sulfur colloid scan or 99mTc-heat–damaged red blood cell scan. Lymphoma is typically homogeneously hypovascular without arterial enhancement.
References: Lewis RB, Lattin GE, Paal E. Pancreatic endocrine tumors: radiologic-clinicopathologic correlation. Radiographics 2010;30(6):1445–1464.
Raman SP, Hruban RH, Cameron JL, et al. Pancreatic imaging mimics: part 2, pancreatic neuroendocrine tumors and their mimics. AJR Am J Roentgenol 2012;199(2):309–318.
4b Answer C.Pancreatic neuroendocrine tumors (NETs) may be nonfunctioning or functioning. Nonfunctioning neoplasms can be asymptomatic or present with symptoms of mass effect because of large size at time of diagnosis. Patients with functioning pancreatic NETs may manifest symptoms of hormonal overproduction as listed in the following table, allowing earlier diagnosis when the tumor is small. The most common functioning subtype is insulinoma, accounting for nearly half of functioning pancreatic NETs. Symptoms of hypoglycemia frequently lead to diagnosis of insulinomas at <2 cm.
Clinical Manifestations of Selected Pancreatic Neuroendocrine Tumors

*VIP, vasoactive intestinal peptide.
NETs typically behave indolently. Curative surgical resection or enucleation is the preferred treatment. Metastatic disease to the liver may be managed with radiofrequency ablation or chemoembolization. Other treatment options include somatostatin analogues (such as octreotide), molecular targeted therapies, and chemotherapy.
References: Lewis RB, Lattin GE, Paal E. Pancreatic endocrine tumors: radiologic–clinicopathologic correlation. Radiographics 2010;30(6):1445–1464.
Sahani DV, Bonaffini PA, Fernández-Del Castillo C, et al. Gastroenteropancreatic neuroendocrine tumors: role of imaging in diagnosis and management. Radiology 2013;266(1):38–61.
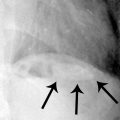
5 Answer C.Diffuse calcifications, seen throughout the pancreas in this case, are specific for chronic pancreatitis. Chronic alcohol consumption accounts for 70% to 90% of cases of chronic pancreatitis in developed countries. Less common causes are chronic biliary tract disease, hereditary pancreatitis, cystic fibrosis, hyperlipidemia, hypercalcemia (most commonly hyperparathyroidism), medications, and pancreas divisum. Chronic pancreatitis, thought to be an entity distinct from acute pancreatitis, is a disease of prolonged inflammation leading to fibrosis and gland dysfunction. Focal or diffuse pancreatic calcifications are present in half of patients, visible on CT and occasionally on radiographs as shown on the following image from a different patient (arrows).

Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


