• Often manifesting before detection of underlying cancer (2/3 of patients)
Median of 12 months from myelopathy onset to cancer detection
• Poor prognosis, often becoming wheelchair dependent
(Left) Sagittal T1 MR shows multiple metastatic lesions involving the cervical and upper thoracic vertebral bodies, with marrow conversion from prior radiation therapy . The cord is mildly expanded.
(Right) Sagittal T2 MR shows longitudinally extensive high signal within the cervical cord, with mild cord expansion . This edema pattern is nonspecific, and cord metastases and radiation change should also be considered.
(Left) Axial T1 C+ MR shows the typical pattern of paraneoplastic myelopathy with focal central tract enhancement in a symmetrical fashion. This symmetrical tract involvement would not be seen with metastases or radiation change.
(Right) Sagittal T1 C+ MR in a patient with a focal cord metastasis shows the very localized nature of the tumor to be contrasted, with the longitudinally extensive abnormality with paraneoplastic disease of the cord.
TERMINOLOGY
Abbreviations
• Paraneoplastic neurologic disorder (PND)
Synonyms
•
Definitions
• Antineuronal immune mechanism targeting CNS, occurring in conjunction with cancer
IMAGING
General Features
• Best diagnostic clue
Longitudinally extensive, symmetric, tract-specific signal changes within spinal cord that often enhance after gadolinium administration in patient with cancer
• Location
Cervical or thoracic cord
• Size
> 3 vertebral segments in length
• Morphology
Linear signal abnormality following spinal cord tract
Radiographic Findings
Only gold members can continue reading. Log In or Register to continue






 involving the cervical and upper thoracic vertebral bodies, with marrow conversion from prior radiation therapy
involving the cervical and upper thoracic vertebral bodies, with marrow conversion from prior radiation therapy  . The cord is mildly expanded.
. The cord is mildly expanded.
 . This edema pattern is nonspecific, and cord metastases and radiation change should also be considered.
. This edema pattern is nonspecific, and cord metastases and radiation change should also be considered.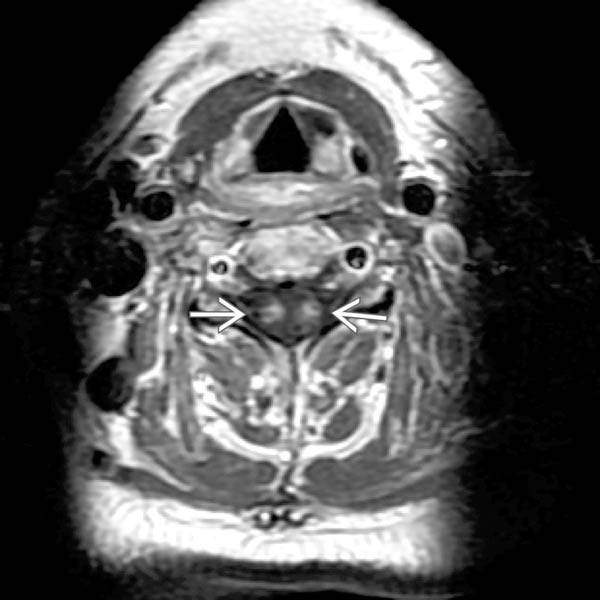
 in a symmetrical fashion. This symmetrical tract involvement would not be seen with metastases or radiation change.
in a symmetrical fashion. This symmetrical tract involvement would not be seen with metastases or radiation change.
 shows the very localized nature of the tumor to be contrasted, with the longitudinally extensive abnormality with paraneoplastic disease of the cord.
shows the very localized nature of the tumor to be contrasted, with the longitudinally extensive abnormality with paraneoplastic disease of the cord.








