Localization: Almost exclusive of the long bones, it originates from the metaphysis. Rare in the diaphyses, exceptional in flat bones. The most typical site is the distal metaphysis of the femur in its posterior aspect (60 % of cases).
Clinical: No or slight pain. There is a bony hard mass. Duration of symptoms not infrequently exceeds 1, 2, or even 5 years. It is not uncommon to see patients having undergone one or more surgical excisions and presenting with a local recurrence.
Imaging: Due to slow growth, parosteal OS is usually seen when it is large. It is a lobulated mass of osseous radiodensity, fused to the cortex with a broad base that tends to wrap around the bone. Radiodensity is maximal near the implant base, while the outer margin tends to be blurred. Detailed radiographies show a mesh of trabeculae (“steel-wool” pattern), from ground glass to ivory density. Toward the diaphysis, the medullary canal is usually not involved. In metaepiphyses, the thin cortex is frequently breached with extension to the cancellous bone. This involvement increases with malignancy and with the standing duration of the tumor and is appreciated by CT in 60 % of cases. CT scan, MRI, and angiography show the tumor adhering to or enwrapping the vascular bundle. Isotope scan is very hot.
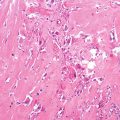
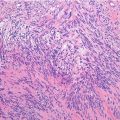
Histopathology: Parosteal OS is composed by spindle cells and collagen fibers embedding osseous trabeculae. Occasionally cartilage may be associated. Cells form long sweeping fascicles with parallel nuclei. Trabeculae appear also as parallel streamers with broken cement lines as pagetic mosaic. Bone is formed by metaplasia from tumor cells (fibro-osseous metaplasia) and trabeculae may not show osteoblastic rimming. Parosteal OS is grade 1 or 2 but may progress in malignancy and transform into a high-grade OS. It is indeed not rare to find areas of different histological grade in the same case. Mets (lung, skeleton) have usually the same pattern as the most malignant part of the primary and are often densely sclerotic.
Course and Staging: The course is usually slow. Parosteal OS is usually staged I-A or B. When histological grade is 3 or 4 (dedifferentiated), the stage is II.
Treatment and Prognosis: Surgery must aim to wide margins. Hemicylindric resection is usually possible in the popliteal region, through a double approach (medial and lateral), elevating the quadriceps. More often, a complete segmental resection of the affected bone is needed. When the tumor impinges on the vascular bundle, wide margins may often require vessel resection and reconstruction. Chemotherapy is only indicated in grade 3 and 4 lesions and it is the same as that used in classic OS. Local recurrence is the rule after intralesional surgery. Mets may be seen in grade 2 and mainly when the underlying bone is invaded. Mets are less common as compared to conventional OS, about 2–10 % in grades 1–2 parosteal OS, but rising to about 60–70 % in grades 3–4 to dedifferentiated parosteal OS.
Key Points
Clinical | Long history of mild symptoms, pain, and swelling |
Radiological
Related posts:Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|