This chapter reinforces concepts presented in this textbook. Students of medicine gather pearls of wisdom from their mentors that may not fit well into a didactic treatment of a subject but are valuable in day-to-day practice. We all learn to avoid pitfalls that arise that have escaped our formal education. Interpretative questions require assembling multiple bits of information for a correct answer, and these questions are not necessarily asked in quite the same way that subject material was presented didactically. This chapter is neither comprehensive nor necessarily weighted toward the relative importance of the topics.
Radiopharmaceuticals
Radiopharmaceuticals are radioactive molecules comprised of a radionuclide that permits external detection and a biologically active molecule or drug that acts as a carrier that determines localization and biodistribution. Exceptions are radioiodine, gallium, thallium, and oxygen-15, in which the radioactive atoms themselves confer the localization properties.
Q : What is the relationship between the half-lives of a parent radionuclide and a daughter radionuclide in a generator system?
A : A longer-lived parent decays to a shorter-lived daughter in all clinical generator systems. The parent radionuclide must have a long enough half-life to permit the formulation and distribution of the generator. The daughter half-life must be long enough for the clinical application.
Q : How are parent and daughter radionuclides separated in generator systems?
A : Because the parent and daughter are different elements, they can be chemically separated (e.g., molybdenum-99 and technetium-99m).
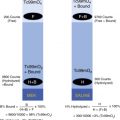
The most common radionuclide contaminant in the generator eluate is the parent radionuclide, Mo-99. Tc-99, the daughter product of the isomeric transition of Tc-99m, is also present but is not considered an impurity or contaminant, although significant Tc-99 can be a problem from a radiolabeling standpoint.
Q : What quality-assurance procedure is used to detect radionuclide impurities?
A : Thin-layer chromatography.
If 5% of a Tc-99m-labeled radiopharmaceutical activity remains as free pertechnetate in a radiolabeling procedure, the radiochemical purity is reported as 95%.
Q : What is the legal limit for Mo-99 in Tc-99m-containing radiopharmaceuticals?
A : The Nuclear Regulatory Commission (NRC) limit is 0.15 microcurie of Mo-99 activity per 1 mCi of Tc-99m activity in the administered dose.
Q : How does the ratio of Mo-99 to Tc-99m change with time?
A : In any preparation in which the radionuclidic contaminants have longer half-lives than the desired radionuclide label, the relative activity of the contaminant increases with time.
Q : What is the purpose of stannous ion in Tc-99m-labeling procedures?
A : Stannous ion is used to reduce technetium pertechnetate from a +7 valence state to lower valence states necessary to allow for labeling a wide range of agents.
Q : What constitutes a medical event, formerly known as a misadministration of a radiopharmaceutical?
A : Previously, a misadministration was defined by the NRC as a radiopharmaceutical given to the wrong patient, receiving the ordered radiopharmaceutical by the wrong route of administration, or the administered dose differing from the prescribed dose by greater than an allowable standard. Although these are all of concern and need reporting within a department and institution, as well as a record of the event, the NRC now requires reporting them only when they are medical events, defined as an event where the effective dose equivalent to the patient exceeds 5 rem to the whole body or 50 rem to an individual organ.
Q : Describe the general response to the spill of radioactive material.
A : The person who recognizes that a spill has occurred should notify all persons in the vicinity, and the area should be restricted. If possible, the spill should be covered. For minor spills, cleanup using appropriate disposable and protective clothing can be accomplished until background or near-background radiation levels are observed. For major spills, the source of the radioactivity should be shielded. For both major and minor spills, all personnel potentially exposed in the area should be surveyed, with appropriate removal of contaminated clothing and decontamination of skin. The radiation safety officer should be notified of all spills and has the primary responsibility for supervising cleanup for major spills and determining what reports must be made to regulatory agencies.
Nuclear Medicine Physics
Positrons are positive electrons, and thus they are particles. With radioactive decay, an emitted positron travels 2 to 10 mm in tissue (depending on the radionuclide) before losing its kinetic energy, then interacts with an electron. The two particles annihilate each other and emit two 511-keV gamma photons at approximately 180-degree angles from each other. The gamma photons can be detected by positron emission tomography (PET) coincidence detectors. This conversion of mass to energy is predicted by Einstein’s well-known formula: E = mc 2 .
Q : What is the difference between x-rays and gamma rays?
A : Both x-rays and gamma rays are ionizing radiation. X-rays originate outside the atomic nucleus; gamma rays originate inside the atomic nucleus. The respective energy spectra for x-rays and gamma rays substantially overlap at the high-energy end of the spectrum for all forms of electromagnetic radiation.
Q : What is the energy equivalent of the rest mass of an electron?
A : The energy equivalent is 511 keV. This is also the energy equivalent of a positron (positive electron).
Q : What is the difference between the rad, roentgen, and rem?
A : These terms are frequently confused with each other but have important distinctions.
The roentgen is defined as radiation exposure, specifically the quantity of x-radiation or gamma radiation that produces 1 electrostatic unit of charge per cubic centimeter of air at standard temperature and pressure. In the International System of Units (SI), radiation exposure is expressed in terms of coulombs per kilogram (C/kg). One roentgen is equal to 2.58 × 10 –4 C/kg air.
A rad, or the radiation absorbed dose, is the traditional unit of absorbed dose equal to the absorption of 100 ergs of energy per gram of absorbing material. The gray (Gy) is the unit of absorbed dose in the SI system; 1 Gy = 100 rads.
The unit rem is an acronym for r oentgen e quivalent m an. The rem is calculated by multiplying the absorbed dose in rads by a factor to correct for the relative biological effectiveness (RBE) of the type of radiation in question. In the SI system, 1 sievert (Sv) = 100 rem.
Q : Which is more penetrating in soft tissues—alpha or beta particles of the same kinetic energy?
A : Alpha particles have very low penetration in soft tissue because of their rapid loss of kinetic energy through the interaction of their electrical charge with electrons in the tissues. Beta particles of the same respective kinetic energy of alpha particles have higher velocity, lower mass, and a single negative charge. They demonstrate considerably greater penetration in soft tissues, although penetration still is typically measured in millimeters.
Q : Define the two systems for expressing radioactive decay.
A : The traditional unit of radioactive decay is the curie (Ci). One curie is equal to 3.7 × 1010 disintegrations per second (dps). This number was derived from the decay rate of 1 g of radium. (Modern measurements indicate that the actual decay rate for 1 g of radium is 3.6 × 1010 dps.) In the SI system, decay is expressed in becquerels (Bcq). One becquerel equals 1 disintegration per second; 1 mCi = 37 MBq.
Q : How are the half-life and the decay constant related?
A : The physical half-life (T ½ ) of a radionuclide is defined as the time for half the atoms in a sample to decay. The T ½ is expressed in units of time, typically seconds, minutes, hours, days, or years. The decay constant indicates the fraction of the sample decaying in a unit of time. The units of the decay constant are “per unit time” (per second, per hour). Mathematically, the T ½ and the decay constant (λ) are related by the following equation: <SPAN role=presentation tabIndex=0 id=MathJax-Element-1-Frame class=MathJax style="POSITION: relative" data-mathml='T12=1n2λ’>T12=1n2λT12=1n2λ
T 1 2 = 1 n 2 λ
Q : After a photon has undergone Compton scattering, how does the energy of the scattered photon compare to the original photon energy?
A : In Compton scattering, the photon gives up energy to a recoil or Compton electron. The “scattered” photon has correspondingly lower energy. The amount of energy lost increases as the angle of scattering increases.
Q : What factors speed up or slow down radioactive decay?
A : Unlike chemical reactions, radioactive decay is a physical constant that cannot be sped up or slowed down by heating or cooling or by applying other physical or chemical influences.
Q : What special term is used to designate the electrons in the outermost shell of an atom?
A : They are called valence electrons and are responsible for many of the chemical characteristics of the element.
Q : What is the binding energy of an electron?
A : Binding energy refers to the amount of energy required to remove that electron from the atom. Electrons in shells close to the nucleus have higher binding energy than electrons farther from the nucleus. This energy is typically expressed in terms of electron volts (eV). The binding energy for each electron shell and subshell is characteristic for the respective element; the higher the atomic number of the element, the greater is the binding energy for each shell and subshell.
Radiation Detection and Instrumentation
Q : What are examples of the uses of ionization chambers in nuclear medicine?
A : Ionization chambers are used for radiation survey meters and some pocket dosimeters. The radionuclide dose calibrator incorporates an ionization chamber.
Q : What is the purpose of the thallium impurity added to sodium iodide crystals in gamma detectors?
A : The thallium is used to “activate” the sodium iodide crystal. The thallium impurity provides “easier” pathways for the return of electrons from the conduction band of the crystal to the valence bands of atoms.
Q : What is the relationship between photon energy and detection efficiency in a sodium iodide crystal?
A : For a given crystal size, detection efficiency decreases with increasing photon energy.
Q : Why do photopeaks appear as bell-shaped curves in pulse height spectra rather than as discrete spikes corresponding to the energy of the gamma ray?
A : Although gamma rays have discrete energies, the detection process is subject to statistical factors at each step of the process. The bell-shaped curve corresponding to the gamma-ray photopeak reflects these statistical variations, which results in different events being measured as having slightly different energies. The better the “energy resolution” of a pulse height analyzer, the narrower the bell-shaped curve.
Q : In using a gamma scintillation camera, what does it mean to “set” the energy window?
A : Gamma cameras are equipped with pulse-height analyzers that allow the operator to select a range of observed energies for accepting photons to be used in making the scintigraphic image. The window is usually described by giving the photopeak energy of interest and a percentage range that defines the limits of acceptance above and below the photopeak energy. A typical window for the 140-keV photon of Tc-99m is 20%, or ±14 keV.
Q : What are the causes of inhomogeneous flood field images in gamma camera quality control?
A : Causes include improper photomultiplier tube voltage adjustment, off-peak camera pulse-height analyzer setting, crystal imperfections or damage, poor coupling of the crystal and the photomultiplier tubes, and inadequate mixing of radiotracer in the flood phantom.
Q : What effects do Compton-scattered photons have on scintigraphic image quality?
A : Compton-scattered photons are the enemy! Scattered photons that fall within the acceptance limits of the energy window are included in the image. They represent false data because they are recorded in a different spatial location than the origin of the primary photon. Thus, Compton scattering reduces image contrast and spatial resolution. Compton-scattered photons falling outside the energy window still must be processed by the gamma camera pulse-height-analyzer circuitry. These rejected events contribute to dead time and reduce the count-rate capability of gamma cameras.
Q : What photons are desired in the scintigraphic image?
A : Primary (unscattered) photons that arise in the organ of interest in the body and travel parallel to the axis of the gamma camera collimator field of view are the photons desired in the image. Intuitively, one may think of these as “good” photons. All other photons are “bad” photons. The good photons include (unscattered) photons that arise in the object or organ of interest but travel “off axis,” primary photons that arise in front of or behind the organ of interest (background photons), and all scattered photons.
Q : What is the purpose of the collimator?
A : The collimator defines the geometrical field of view of the gamma camera crystal. Off-axis photons, whether they are primary photons or scattered photons, are absorbed in the septa of the collimator and do not get to the crystal.
Pinhole collimators allow resolution of objects below the spatial resolution of the gamma camera through geometrical magnification.
Q : What is the construction difference between a low-energy, all-purpose collimator and a low-energy, high-resolution collimator?
A : A high-resolution collimator has more holes that are smaller and deeper.
Q : How does poor energy resolution degrade spatial resolution?
A : Gamma cameras with poor energy resolution have reduced ability to reject scattered photons on the basis of pulse-height analysis, as well as reduced ability for accurate determination of x – and y -coordinates for spatial localization of events.
Single-Photon Emission Computed Tomography and Positron Emission Tomography
Most nuclear medicine imaging clinics use 180-degree single-photon emission computed tomography (SPECT) acquisition for cardiac studies and 360 degrees for imaging most other organs, including the brain.
For SPECT imaging, the highest-resolution collimator that provides sufficient count rate should be selected, usually the high-resolution parallel-hole collimator.
In addition to equipment factors, patient motion is the most important cause of image degradation in SPECT and positron emission tomography (PET) studies.
Q : What special importance does the biological half-life of a radiotracer have in SPECT imaging?
A : In SPECT imaging, two-dimensional data are acquired from sequential sampling angles. If significant biological change in the distribution of a radiopharmaceutical takes place between the start of data acquisition and completion, the reconstruction of tomographic images can be significantly distorted.
Q : What is a filter?
A : Filters are special mathematical functions applied to SPECT and PET data that enhance desired characteristics in the image, such as background subtraction, edge enhancement, and suppression of statistical noise. A ramp filter is designed to eliminate or reduce the star artifact during reconstruction.
With SPECT and PET, flexible reformatting of image data can be performed in multiple image planes, typically transverse, coronal, and sagittal. For cardiac imaging, short-axis, vertical long-axis, and horizontal long-axis views of the heart are typically obtained.
Two quick ways of assessing patient motion during SPECT imaging are to view the projection images as a cinematic closed-loop display or to create slice sinograms. In the cinematic display, patient motion is seen as a change in position from one projection image to another. It best shows vertical motion. On sinograms, patient motion is seen as a discontinuity in the stacked projection profiles.
SPECT is subject to various artifacts. Field flood nonuniformity can result in ring artifacts. Center-of-rotation misalignment results in loss of image resolution and, if severe, also ring artifacts.
The spatial resolution of PET is twice or greater than that of SPECT.
Spatial resolution in PET is limited by positron travel distance in soft tissue before annihilation and photon emission.
PET imaging with transmission attenuation correction and detector sensitivity calibration allows for absolute quantitative uptake determinations.
Positron emitters, such as carbon, nitrogen, oxygen, and fluorine (as a replacement for hydrogen), make possible the potential radiolabeling of any biological compound. However, the chemistry for developing and radiolabeling single-photon radiopharmaceuticals can be complex.
Endocrine
Q : What is the origin of lingual and sublingual thyroid tissue?
A : The main thyroid anlage begins as a down-growth from the foramen cecum. Thyroid tissue may be seen anywhere along the tract of the thyroglossal duct from the foramen cecum to the usual location of the gland. However, with lingual thyroid tissue, usually a failure of normal development occurs, with no tissue in the normal location of the thyroid.
Q : What is the difference in mechanism of thyroid uptake between Tc-99m pertechnetate and radioiodine?
A : Radioiodine is taken up or extracted (trapped) by the thyroid follicular cell and organified, binding to tyrosine residues on thyroglobulin, and stored in the colloid of the follicle. Tc-99m pertechnetate is trapped but not organified.
Q : What has happened to the range for normal percent thyroid uptake of radioiodine in the United States over the last 50 or more years?
A : The normal range has dropped significantly as a result of iodination of salt and the use of iodine in foods. The normal 24-hour range was 20% to 45% in the 1960s but is now 10% to 30%.
Radioiodine is administered orally. Tc-99m pertechnetate is administered intravenously.
A potentially serious pitfall is to confuse microcuries with millicuries.
The following are the approximate adult doses of iodine-123 and iodine-131 used for uptakes, scans, and therapy. Serious consequences can result from confusing these doses, particularly if a therapeutic dose is administered instead of a diagnostic dose.
I-123 uptake (50–100 microcuries [μCi])
I-123 scan (200–400 μCi)
I-131 uptake (10 μCi)
I-131 scan substernal goiter (50 μCi)—however, I-123 has replaced I-131 for this indication
I-131 therapy for Graves disease (7–15 millicuries [mCi])
I-131 therapy for thyroid cancer (30–200 mCi)
Q : What is the normal distribution of radioiodine and Tc-99m pertechnetate?
A : Radioiodine is taken up by the thyroid, salivary glands, and stomach and excreted by the kidneys. Tc-99m pertechnetate has identical uptake and clearance, except that because it is not organified, it remains in the thyroid and salivary glands for a much shorter time.
After injection of the radiopharmaceutical, Tc-99m pertechnetate scans are acquired at 15 to 20 minutes. Routine I-123 thyroid scans after oral ingestion are acquired at 4 hours. The delayed imaging for I-123 is to allow background clearance. Tc-99m is not organified like I-123; thus, it must be imaged earlier because of the rapid thyroid washout.
Q : What are common causes of falsely low thyroid uptakes?
A : Patients taking thyroid hormones, iodine-containing drugs, organification blockers such as propylthiouracil or methimazole, and recent administration of intravenous iodine-containing radiographic contrast are common causes.
A thyroid scan should not be performed within 6 to 8 weeks of the patient receiving a CT scan with intravenous iodine contrast.
Q : How does the methodology differ for a thyroid scan and thyroid uptake?
A : A thyroid uptake is a nonimaging study using a gamma-detector counting probe, whereas a thyroid scan results from gamma camera imaging.
Swallowed activity from salivary secretions on Tc-99m pertechnetate or radioiodine scans occasionally remains in the esophagus and can confuse interpretation. The nature of the activity can be determined by having the patient drink water, followed by reimaging of the neck.
Q : How can a thyroid uptake test differentiate the two most common causes of thyrotoxicosis, Graves disease, and subacute thyroiditis? Why?
A : In the initial phase of subacute thyroiditis, thyroid hormones are released from the inflamed gland, causing thyrotoxicosis. Both radioiodine and Tc-99m uptake require thyroid-stimulating hormone (TSH) stimulation for uptake. As a result of pituitary feedback of elevated serum thyroid hormones, TSH is suppressed. Thus, the uptake of radioiodine or Tc-99m pertechnetate is suppressed. With Graves disease, although TSH is suppressed, the gland is autonomous, and the uptake is high.
Q : What is the mechanism of action of antithyroid drugs propylthiouracil (PTU) and methimazole (Tapazole)?
A : Both are thiourea antithyroid drugs that block the organification of iodine.
Q : What medical conditions are associated with an increased incidence of pheochromocytomas and paragangliomas?
A : Both forms of multiple endocrine neoplasia type II are associated with pheochromocytoma, as are von Hippel–Lindau disease and neurofibromatosis.
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


