Pelvic Fractures
- Howard J. O’Rourke
- Georges Y. El-Khoury
Osseous Emergencies
Mechanisms and Patterns of Fractures of the Pelvis
The pelvis is a complex series of articulations supported by a strong ligamentous network. The posterior ligaments are the strongest ( Fig. 16-1 ). The sacroiliac joint has thin anterior and thick posterior ligaments. The sacrospinous and sacrotuberous ligaments are additional posterior ligaments that primarily serve to resist rotational deformity of the pelvis. The pubic symphysis is supported by a series of comparably weaker ligaments.

Pelvic fractures are a potentially devastating injury encountered in emergency medicine with an overall mortality reported between 8% and 17%. Fractures of the pelvis may be classified as stable or unstable; with unstable fractures the pelvic ring is disrupted, particularly posteriorly. The most common cause of mortality is hemorrhage, which may be arterial, venous, or bleeding from fractured cancellous bone. The most widely used classification system is the Young-Burgess system, which seeks to classify fractures based on the vector of force at the time of injury.
Radiology plays a central role in the classification and management of pelvic ring disruption. A strict approach to the pelvic radiograph will help in identifying and classifying fracture patterns. One’s search pattern in a trauma patient should evaluate the iliopectineal and ilioischial lines as well as the obturator and pelvic rings ( Figs. 16-2 and 16-3 ). The sacroiliac joints and pubic symphysis should also be evaluated for widening and craniocaudal displacement.


According to the classification system proposed by Young and colleagues, fractures are defined as lateral compression, anteroposterior compression, vertical shear, and combined mechanical injury. Lateral compression and anteroposterior injuries are further subdivided into types I to III depending on severity of injury ( Table 16-1 ).
| Fracture Type | Description |
|---|---|
| Lateral compression—internal rotation injuries | I—Compression fracture of sacrum |
| II—Iliac wing fracture | |
| III—Contralateral open-book injury | |
| Anteroposterior compression—external rotation injuries ∗ | I—Stretched but intact anterior sacroiliac, sacrospinous, and sacrotuberous ligaments |
| II—Torn anterior sacroiliac ligaments with intact posterior ligaments | |
| III—Complete ligamentous disruption | |
| Vertical shear | Diastasis of symphysis or vertical rami fractures with vertical displacement at either sacroiliac joint, iliac fracture, or sacral fracture |
| Combined mechanism | Combined other patterns |
Lateral compression (LC) injuries represent the most common type of pelvic ring fracture. So named for the direction of force, there is resultant internal rotation of the iliac bone ( Fig. 16-4 ). In LCI fractures the fractures of the rami are horizontal and overlapping. The posterior ring injury most often is a buckle fracture of the sacrum. Given the stability of the sacrospinous and sacrotuberous ligaments, the pelvis remains vertically stable ( Fig. 16-5 ). In LCII fractures the iliac wing fractures, and the fracture may extend posteriorly to the sacroiliac joint. LCIII fractures are LCI or LCII on the side of injury and a contralateral open-book injury. The mechanism is internal rotation on the side of injury and external rotation on the contralateral side. The contralateral side may show partial or complete disruption of the sacroiliac joint. LCIII injuries are rotationally and possibly vertically unstable.


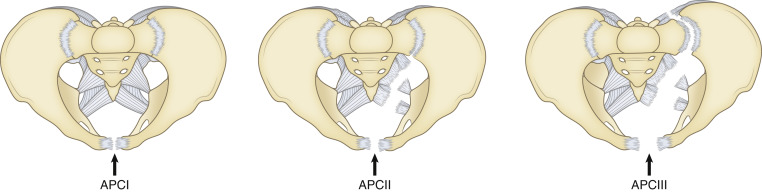
Anteroposterior compression (APC) injuries account for 15% to 20 % of all pelvic ring injuries. The vector of force leads to diastasis of the symphysis pubis with or without diastasis of the sacroiliac joint or fracture of the iliac bone. APCI injuries show less than 2 cm widening at the pubic symphysis and little to no widening of the sacroiliac joint. Vertical rami fractures may be seen. More severe APC injuries cause disruption of the sacroiliac joint, ranging from either anterior widening to disruption of the entire joint ( Fig. 16-6 ). Complete separation of the hemipelvis precludes the tamponade of vascular injury. The proximity of the superior gluteal arteries and internal pudendal arteries to the sacroiliac joint contributes to the incidence of significant hemorrhage with APC injuries ( Figs. 16-7 and 16-8 ).


Vertical shear injuries occur because of axial loading of the pelvis, as with a fall from height on an extended leg ( Fig. 16-9 ). Characteristic radiographic findings include vertical rami fractures or diastasis of the symphysis and dislocation of the sacroiliac joint or sacral fracture. Furthermore, the hemipelvis displaces superiorly and posteriorly. In combined mechanical injuries, a combination of two or more vectors results in complex pelvic fractures ( Fig. 16-10 ).


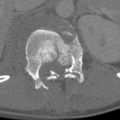
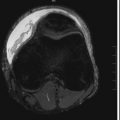
Sacral Fractures
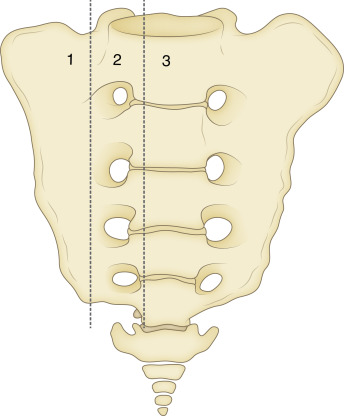
Sacral fractures are an important yet difficult-to-recognize injury. Mechanistically injuries can be associated with high-energy trauma or simply normal stress on insufficient bone. The most widely used system for describing sacral fractures was created by Denis and coworkers in 1988 ( Fig. 16-11 ). The sacrum is divided into three zones. Zone 1 fractures involve the region of the sacral ala; L5 is occasionally injured with zone 1 fractures. Zone 2 fractures involve the region of the sacral foramina. These frequently cause sciatica and rarely bladder dysfunction. Zone 3 fractures occur more centrally, and the patients experience saddle anesthesia and sphincter dysfunction.
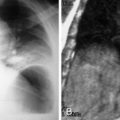
Radiographs are relatively insensitive in detecting sacral fractures due to significant overlying soft tissues and bowel gas. Radiologists should be sensitive to the disruption of sacral ala on anteroposterior (AP) pelvis radiographs. A bone scan is very sensitive to the presence of a sacral insufficiency fracture ( Fig. 16-12 ). Fractures are optimally characterized at computed tomography (CT). Traumatic sacral injuries frequently occur in association with other pelvic fractures.