The periosteum is a membrane that covers the majority of bone except at locations at and near cartilage. How periosteum responds to stimuli (e.g., trauma, infection, metabolic process, and neoplasm) can often give clues to the etiology of the underlying stimulus. An aggressive or destructive process will often greatly alter the periosteum, whereas a nonaggressive process usually gives the periosteum the opportunity to remodel with a more orderly architecture. The distribution of periosteal reaction (focal or diffuse) may give clues to the underlying process. Periosteal reaction may also be grouped into several patterns: smooth, solid or thick, and aggressive (laminar, sunburst, Codman triangle, and cloaking).
Smooth periosteal reaction consists of one or multiple unbroken layers of ossified periosteum along the cortical surface. Smooth periosteal reaction indicates orderly new bone formation; the bone has had time to heal or remodel toward its original architecture. As a rule, the unbroken lamellar reaction suggests a process that is not very aggressive.
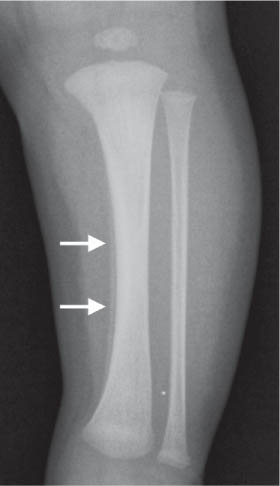
Smooth symmetric periosteal reaction of rapidly growing bones.
Typically involves rapidly growing bones: femur, tibia, and humerus. Symmetric distribution and age (newborn) also support this diagnosis.
Healing fracture or infection
Smooth periosteal reaction at and adjacent to the injury.
Often seen in plastic/bowing fractures.
Margins of an aggressive process
The periosteum at margins of an aggressive process may be less affected than at the site of maximal destruction. The lesion should be classified based on the more aggressive features.
Vascular insufficiency
Periostitis of affected limb (s).
Especially venous stasis.
Hypertrophic osteoarthropathy
Symmetric periostitis of the radius and ulna > femur, humerus, metacarpals, and metatarsals.
Associated with underlying cardiopulmonary diseases (e.g., cystic fibrosis), infection, and malignancy. Adults > children. Digital clubbing. May affect a single extremity in arterial infections.
Early stage: symmetric subperiosteal new bone formation along the diaphyses of the extremities, hands, and feet. Advanced stage: diffuse subperiosteal bone formation, ossification of ligaments and tendons, ankylosis, acroosteolysis.
Rare hereditary disorder: Digital clubbing, thickened skin, and periostosis. Increased uptake along cortical margins on bone scan.
Fig. 5.163 Benign periosteal reaction of the newborn (arrows).
Table 5.82 Periosteal reaction: solid or thick new bone formation
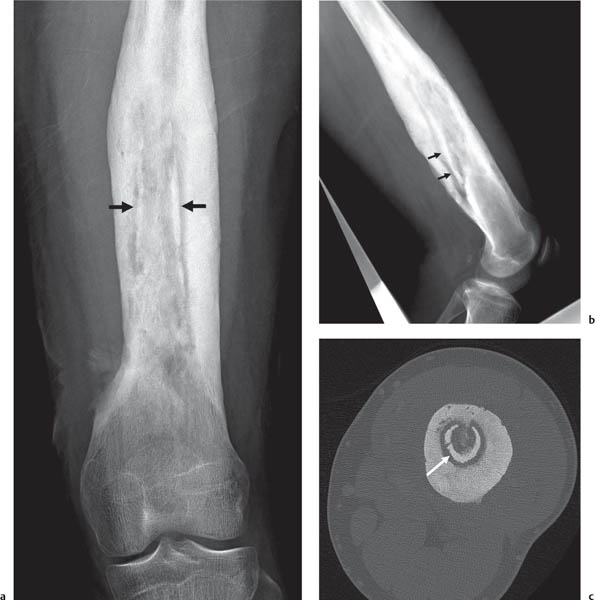
Fig. 5.164a–c Chronic osteomyelitis with thick irregular periosteal reaction enveloping a sequestrum (arrows) on radiography (a, b) and CT (c).
Aggressive periosteal reaction is likely the result of disorganized new bone in response to a destructive process. New bone formation cannot keep pace with the accelerated rate of bone destruction. In response to a rapidly destructive process, new bone formation along the periosteum produces several characteristic patterns. Lamellar (onion peel) periosteal reaction appears as successive layers of new bone arising from the periosteal surface. Spiculation is caused by calcification of the periosteal Sharpey fibers, which are oriented perpendicular to the cortical surface. The radial sunburst pattern is a classic sign of osteosarcoma and affects mainly mineralized osteoid. However, the sunburst pattern may also be seen in hemolytic anemias, thalassemia, and sickle cell anemia. The Codman triangle is another sign indicating an aggressive process. The Codman triangle is an acutely-angled triangle of periosteal reaction along the cortex surface and indicates the transition between the periosteum of the aggressive disease process and the uninvolved bone. No tumor cells are found in the Codman triangle. Just as the physis will act as a temporary barrier to the spread of tumor or infection, the periosteal collar will remain intact.
Table 5.83 Periosteal reaction: aggressive (laminar, sunburst, and Codman triangle)
Bone destruction with varying types of periosteal reaction: Codman triangle, cortical and periosteal destruction, and disorganized periosteal new bone formation.
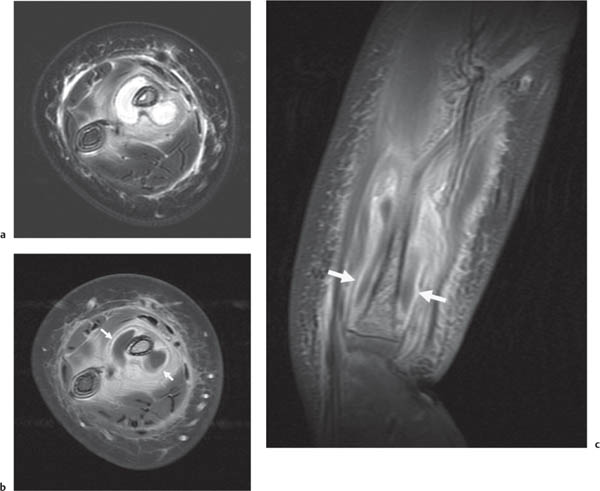
Fig. 5.165a–c Acute osteomyelitis and subperiosteal abscess formation. Fluid has developed deep to the periosteum (arrows in b and c) around the radius on T2-weighted (a) and enhanced T1-weighted (b, c) MRI.Fig. 5.166 Thalassemia. Hair-on-end appearance of the skull (arrows).Fig. 5.167 Sickle cell disease with aseptic dactylitis. Periostitis layers along the diaphysis (arrow).Fig. 5.168 Metastatic neuroblastoma with moth-eaten pattern of lytic bone destruction in the femoral diaphysis and distal metaphysis.
Periosteal cloaking occurs when a long segment of periosteal membrane is altered by disease and results in a long segment of exuberant thickening. Rapidly growing bones appear to be predisposed to producing cloaking in response to injury. Trauma and infection are the most common causes of cloaking.
Usually after trauma. May be seen in neurofibromatosis type 1 or hemophilia after minor trauma, which leads to chronic dysplastic changes in the bone.
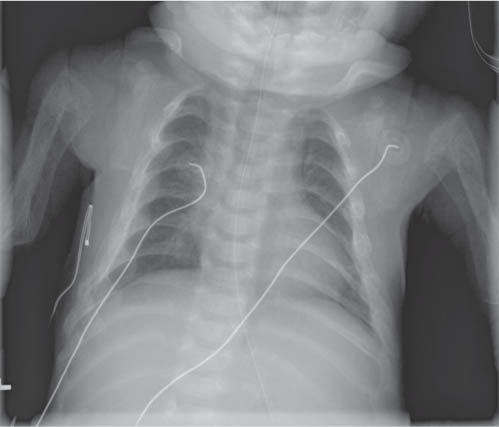
Prostaglandin therapy
Periosteal elevation early in treatment (9–11 d) followed by cloaking.55 Periosteal elevation is relatively common in infants treated with prostaglandins. After cessation of therapy, the periostitis resolves and the bones normalize.
Subperiosteal cortical hyperostosis. Epiphyses spared. Fever and soft-tissue swelling adjacent to involved bones. Rarely appears after 5 mo and usually resolves spontaneously by 2 y. Imaging appearance will depend on phase of disease.
Table 5.85 Periosteal reaction: fluffy or indistinct
Diagnosis
Comments
Metabolic
Appearance of periosteum will depend on the stage of treatment.
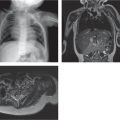
Fig. 5.169 Mucopolysaccharidosis II (Hunter syndrome). Severe osteopenia, widened ribs, and periosteal reaction including cloaking that involves the ribs and humeri.
Table 5.86 Periosteal reaction: focal
Diagnosis
Comments
Trauma
Appearance will vary depending on the stage of healing.