Fig. 9c.1
Setting up the scan protocol. The different “Exam Protocol Groups” are shown in Panel A while Panel B details the “Cardiac Exam Protocols” such as “Coronary CTA”. Depending on the planned examination, you can select between different protocols (e.g., standard helical “Coronary CTA,” “Step & Shoot” mode, or “Calcium Scoring”)
Each examination starts with a surview (scanogram) to determine the position of the heart. The localizer scan should be as small as possible while covering the entire heart and is acquired during a single inspiratory breath-hold. The scan area for a standard coronary CT angiography is often determined using the tracheal bifurcation as the upper reference point. It is also the level of the plane in which the tracker for the bolus timing algorithm is placed. The scan ends about 1–2 cm below the heart (Fig. 9c.2). The scanner gantry isocenter line should be properly placed in the center of the heart. Finally, the entire heart is examined with ECG gating during a single inspiratory breath-hold.
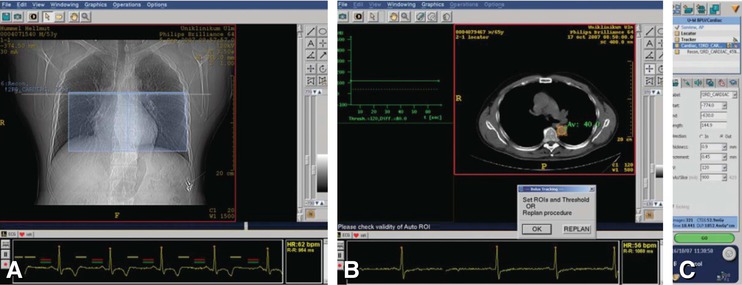
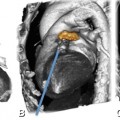
Fig. 9c.2
The user interface for a standard retrospective helical scan, including the defined field of view and an ECG viewer, is shown in Panel A. The blue box indicates the preselected scan area and range. For bolus tracking, the ROI is positioned in the descending aorta (Panel B). The dose indication box shows the expected dose exposure and scan time (Panel C)
The scan is timed to coincide with peak contrast enhancement, derived from the preceding bolus tracking. Bolus tracking is performed by a Locator and a Tracker scan, positioned on the level of the tracheal bifurcation. Pressing “Go” starts the Locator scan, and the system automatically shows the tracker window. A region of interest (ROI) is positioned in the descending aorta (Fig. 9c.2). Now bolus tracking and injection of contrast medium must be started at the same time. After a start delay, several transverse sections are successively acquired at the defined level. The scan starts automatically once attenuation enhancement values in Hounsfield units reach a predefined threshold.
9.2 Prospective Axial Acquisition (“Step & Shoot”)
Since the introduction of the new scanner generation (Brilliance iCT) with a rotational speed of 270 ms and a detector width of 8 cm (128 rows), the majority of patients (80–90%) can be scanned with prospective axial acquisition (“Step & Shoot”) with helical retrospective gating being reserved for data acquisition in patients with arrhythmia and high heart rates. As a prospectively gated scan mode, “Step and Shoot” requires a stable heart rate below 70 beats per min. This scan type combines the advantages of axial and helical scans and relies on sequential axial acquisition. Generally, “Step & Shoot” involves a typical scan sequence that is based on volume acquisition (“Shoot”) and table movement (“Step”). Depending on the system used, the heart is covered in four to six (Brilliance 64) or two to three (iCT) axial rotations, combined with prospective triggering (Fig. 9c.3). The main advantages of “Step & Shoot” scanning are summarized in List 9c.1.
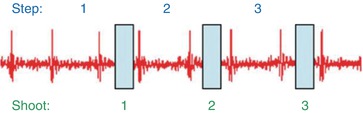
Fig. 9c.3
The principle of sequential axial acquisition after table movement (Step), combined with prospective ECG gating (triggering)
List 9c.1. Advantages and disadvantages of prospective coronary acquisition
Advantages:
1.
Provides a low-dose scan with a dose reduction to one-fourth of that of standard helical scans
2.
Image quality is comparable (or even better with the iCT) to that of standard helical scans
3.
Improved rotational speed of the iCT enables coverage of the whole chest in one breath-hold with “Step & Shoot”; e.g., to image coronary artery bypass grafts or to perform a triple rule-out scan
4.
Allows each volume to be reconstructed from a single cardiac cycle resulting in a better edge depiction of the coronary arteries
5.
Includes an online arrhythmia handling mechanism (Fig. 9c.4)
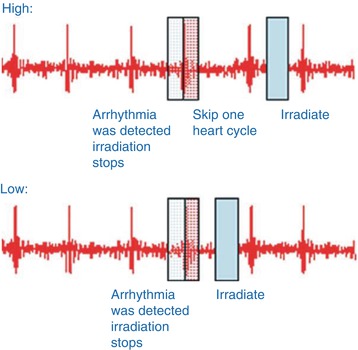
Fig. 9c.4
Two options are available for online arrhythmia handling in the “Step & Shoot” mode. “High” arrhythmia tolerance: When an arrhythmia is detected, irradiation stops immediately; the system waits for one cardiac cycle and then continues exposure in the same table position after the next cycle. “Low” arrhythmia tolerance: When an arrhythmia is detected, irradiation stops immediately; the system continues exposure in the same table position in the cycle immediately following. To prevent excessively long scan times (in the “High” tolerance mode), in a sequence of more than two irregularities, the “High” strategy is automatically changed to “Low”
Disadvantages:
1.
Limited to patients with stable heart rates below 70 beats per min
2.
Lower temporal resolution when compared to helical scans
3.
Geometric distortion at the borders of the prospectively acquired slabs (Fig. 9c.5)Get Clinical Tree app for offline access
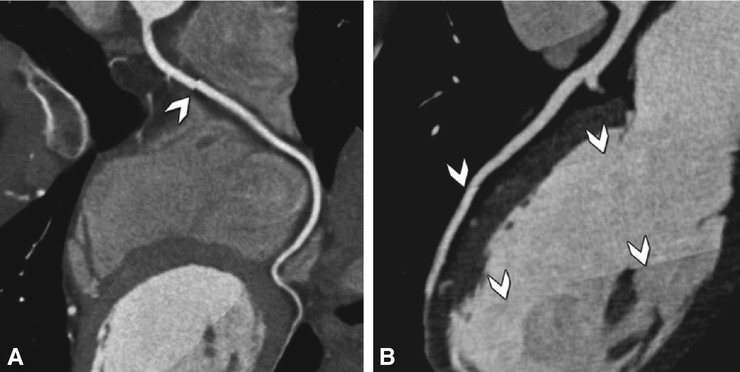
Fig. 9c.5
Drawbacks of the “Step & Shoot” approach. Curved multiplanar reformations of the right coronary artery with “steps” (arrowheadRelated posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree