Air-space or alveolar consolidation
Linear or septal
Reticular
Nodular
Reticulonodular
Ground-glass opacity
Water (e.g., pulmonary edema)
Blood (e.g., pulmonary hemorrhage)
Pus (e.g., pneumonia)
Cells (e.g., bronchioloalveolar carcinoma, lymphoma, eosinophilic pneumonia, organizing pneumonia (also known as bronchiolitis obliterans or BOOP), hypersensitivity pneumonitis, interstitial pneumonia)
Other substances (e.g., lipoprotein in alveolar proteinosis, lipid in lipoid pneumonia)
TABLE 10.1 Linear or Septal Pattern: Differential Diagnosis | ||||
|---|---|---|---|---|
|
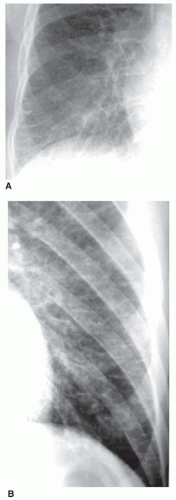 FIG. 10.1. Kerley B lines. Coned-down views of the right (A) and left (B) lateral costophrenic angles in two different patients with cardiogenic interstitial pulmonary edema. Thin horizontal lines in the lung periphery represent Kerley B lines. These represent thickened interlobular septa. |
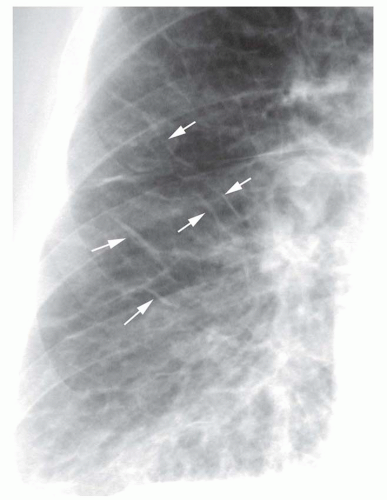 FIG. 10.2. Kerley A lines. A patient with pulmonary edema associated with fluid overload shows multiple Kerley A lines. Thin oblique lines in the parahilar lung (arrows) represent A lines. Thickening of the minor fissure also is seen. |
lines in patients with fibrosis are seen most commonly in patients with sarcoidosis.
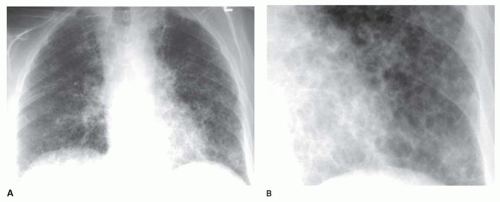 FIG. 10.3. Reticular pattern in rheumatoid lung disease. A: Chest radiograph shows decreased lung volumes and irregular reticular opacities at the lung bases. Kerley B lines are inconspicuous. The lines appear to outline spaces 1 cm or less in diameter, representing a medium reticular pattern. B: Coned-down view of the left lower lobe in the same patient shows the irregular reticular pattern. |
TABLE 10.2 Reticular Pattern: Differential Diagnosis | ||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||
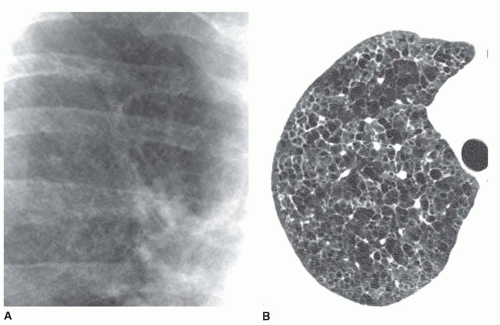 FIG. 10.4. Fine reticular pattern in Langerhans’ cell histiocytosis. A: Coned-down view of the right upper lobe shows fine reticular opacities with poor definition of pulmonary arteries. B: HRCT shows cystic disease. Superimposition of the cyst walls results in the fine reticular pattern that is visible on chest radiographs. |
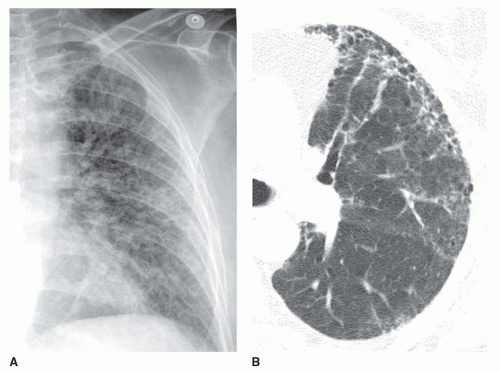 FIG. 10.5. Medium reticular pattern in rheumatoid lung disease. A: Chest radiograph shows irregular reticular opacities, best classified as a medium pattern. B: HRCT shows reticular opacities associated with honeycombing in the anterior lung. |
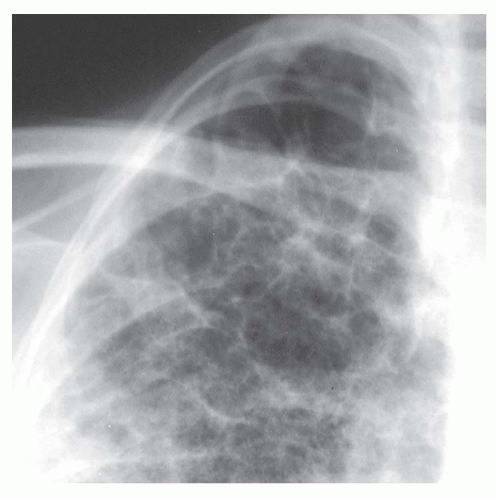 FIG. 10.6. Coarse reticular pattern in cystic lung disease. Coned-down view of the right apex shows reticular opacities outlining spaces exceeding 1 cm. |
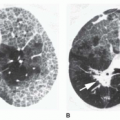
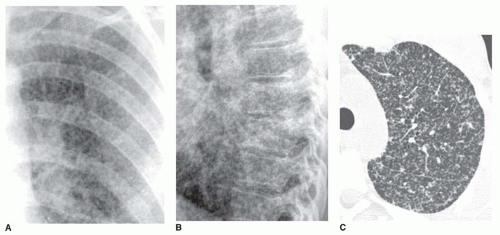 FIG. 10.7. Miliary nodules in hematogenous spread of coccidioidomycosis. Coned-down views from PA (A) and lateral (B) radiographs show innumerable nodules a few millimeters in diameter. C: HRCT shows innumerable, very small lung nodules. |
tuberculosis and fungus), noninfectious granulomatous diseases (e.g., sarcoid, histiocytosis, hypersensitivity pneumonitis), and some pneumoconioses (primarily silicosis and coal worker’s pneumoconiosis [CWP]). Metastases tend to have a basal predominance because of greater blood flow to the bases (see Fig. 10-9); the granulomatous diseases and pneumoconioses, for a variety of reasons, often have an upper lobe predominance.
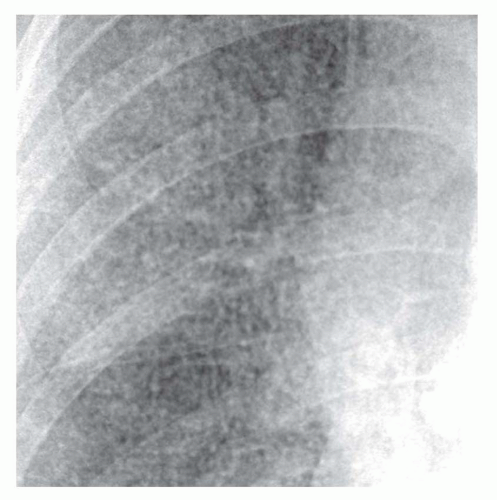 FIG. 10.8. Miliary tuberculosis. Coned-down view of the right upper lobe shows innumerable, discrete, very small nodules. |
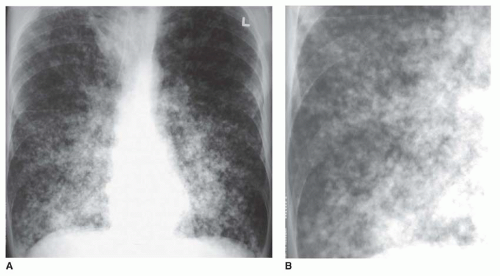 FIG. 10.9. Small nodules in metastatic melanoma. A: Numerous small nodules are visible, with a basal predominance. B: Detailed view of the right lower lobe shows small nodules. |
but this abnormality can be quite subtle and difficult to diagnose with certainty. It is a nonspecific pattern (see the following section on HRCT) and can be seen in the presence of either air-space disease or interstitial disease. Because it is nonspecific, its differential diagnosis is very long. It may be seen with edema, hemorrhage, infections, and a wide variety of different DILDs. When visible on a chest film, it is best evaluated by assessment of the history and clinical presentation in patients with acute symptoms or by further imaging (e.g., HRCT) in patients with chronic symptoms (see Fig. 10-11B).
TABLE 10.3 Nodular Pattern: Differential Diagnosis | |||||||||
|---|---|---|---|---|---|---|---|---|---|
|
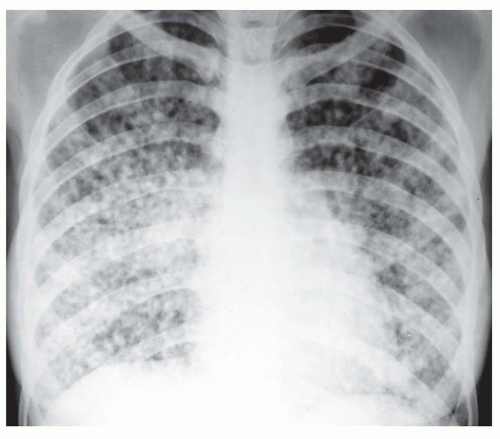 FIG. 10.10. Endobronchial spread of tuberculosis. Ill-defined nodules ranging from 5 to 10 mm in diameter are visible. |
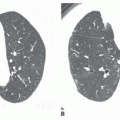
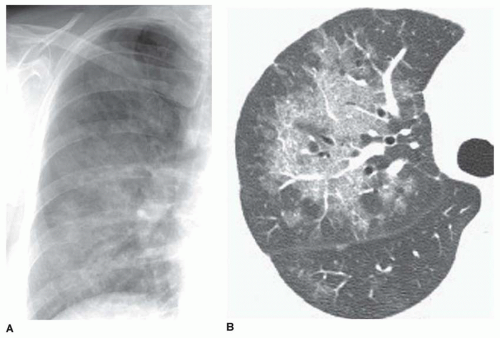 FIG. 10.11. Ground-glass opacity in exogenous lipoid pneumonia. A: Chest radiograph shows a subtle increase in lung opacity in the right parahilar region. Pulmonary vessels are poorly defined. B: HRCT coned down to the right lung shows patchy ground-glass opacity. |
(1.5 mm or less) and a high-resolution algorithm for image reconstruction is essential.
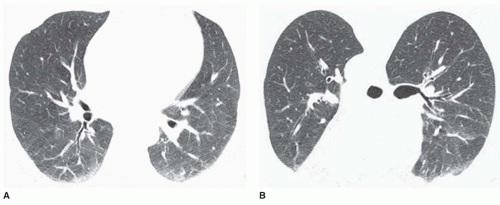 FIG. 10.12. Normal dependent lung collapse and the use of prone scans. A: Supine HRCT in a normal subject shows increased opacity in the posterior (dependent) lung. This appearance cannot be distinguished from lung disease. B: Prone scan shows that the posterior lung is normal. |
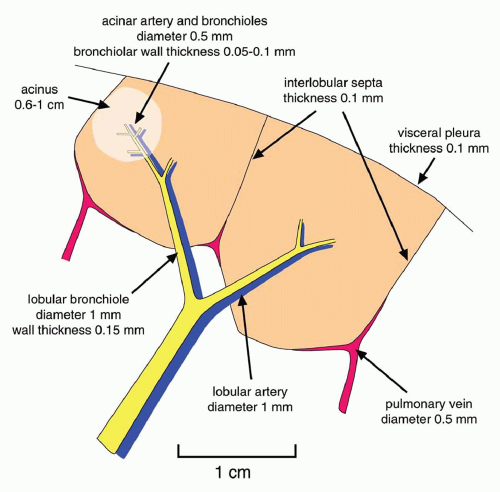 FIG. 10.13. Normal anatomy of the pulmonary lobule. Two lobules are shown. |
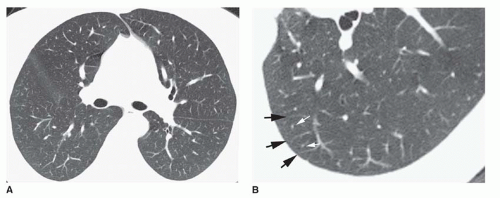 FIG. 10.14. Normal HRCT. A: The lung appears homogeneous in attenuation, with the posterior lung appearing slightly denser than the anterior lung. Fissures are smooth and uniform in thickness. Vessels are smooth in contour and sharply marginated. The most peripheral vessels visible are 5 to 10 mm from the pleural surface and represent centrilobular arteries or, sometimes, veins in interlobular septa. Centrilobular bronchioles and interlobular septa are not visible. B: Coned-down HRCT of the left lower lobe. Two pulmonary lobules are outlined by pulmonary veins within interlobular septa (black arrows). Centrilobular arteries are visible as dots (white arrows). |
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


