TABLE 7.1 Advantages and Disadvantages of Imaging Modalities for Evaluating Pleura | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
 FIGURE 7.1 Layering pleural effusion in an 11-year-old boy with pneumonia. A: Frontal radiograph shows opacity at the right lower lobe most likely representing a consolidation (asterisk). However, an underlying pleural effusion cannot be completely excluded. B: Subsequently obtained right lateral decubitus radiograph confirms the presence of a layering pleural effusion (arrows). C: Ultrasound image shows anechoic fluid (asterisk) above the diaphragm, between the liver and the lung. |
 FIGURE 7.2 Pleural effusion in a 20-month-old girl. A: Frontal radiograph shows complete opacification of the left hemithorax (asterisk) with mediastinal shift to the contralateral side (right side). B: Ultrasound image demonstrates a complex pleural effusion with multiple internal septations (arrows). |
problem-solving in specific situations when further characterization of the pleural lesions is necessary after other imaging studies. Various signal characteristics on MRI can help diagnose pleural disease and help differentiate benign from malignant pleural processes. However, histologic evaluation is often ultimately necessary for a definitive diagnosis (Fig. 7.5). MRI examinations for evaluation of the pleura mainly consist of T1- and T2-weighted MR images, as well as postcontrast T1-weighted MR images in axial and coronal planes. MR images in sagittal plane can be useful for assessing pleural abnormalities adjacent to the sternum or spine.
 FIGURE 7.3 Lung abscess in a 33-month-old boy with pneumonia. Contrast-enhanced coronal reformatted CT image shows a round low-attenuation fluid collection (asterisk) centered within the left lower lobe with peripheral contrast enhancement most consistent with a lung abscess. |
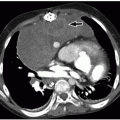
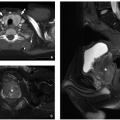
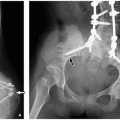
 FIGURE 7.4 Pleural metastasis in a 16-year-old boy with testicular cancer. A: Contrast-enhanced axial CT image shows multiple enhancing pleural-based masses (arrows) with adjacent pleural effusion (E) and consolidation of the left lower lobe (asterisk). B: Contrast-enhanced axial CT image of the lower pelvis demonstrates a heterogeneously enhancing left testicular mass (arrow). |
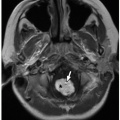
 FIGURE 7.5 Pleural metastasis in a 15-year-old boy with synovial cell sarcoma. Axial T2-weighted MR image shows multiple low-signal pleural-based masses (asterisk) in the right hemithorax. (L, lung; E, pleural effusion.) |
recent intervention, such as a lung biopsy, thoracentesis, or mechanical ventilation.5 Iatrogenic pneumothorax can be also secondary to blunt or penetrating trauma, with or without an associated rib fracture (Fig. 7.9). Air can be introduced into the pleural space not only from an external wound but also secondary to pulmonary, esophageal, or tracheobronchial injuries.
 FIGURE 7.6 Normal pleural anatomy. Schematic diagram of the lungs shows the parietal pleura outlining the chest wall and the visceral pleura overlying the lung as well as invaginating into the different fissures. The parietal and visceral pleural are continuous (pleural reflections) creating the potential pleural space. |
 FIGURE 7.7 Normal pleural anatomy. The lymphatics of the parietal pleura produce the majority of the pleural fluid, which is exuded into the pleural space via stomata. The mesothelial cells secrete a surfactant-like substance that lubricates the pleural cavity. |
 FIGURE 7.8 Spontaneous pneumothorax in a 15-year-old boy who presented with acute shortness of breath and right-sided chest pain. Coronal reformatted lung window CT image shows a large right pneumothorax with collapse of the right lung. Also noted are small blebs (arrow) at the right lung apex most likely the cause of this patient’s spontaneous pneumothorax. |
 FIGURE 7.9 Traumatic pneumothorax in an 8-year-old boy status post motor vehicle accident. Axial lung window CT image shows a left pneumothorax (asterisk). Opacities in the left lung are consistent with lung contusions with pneumatoceles (arrows) containing fluid (hemorrhage). |
patients, a cross-table lateral radiograph or decubitus radiograph can be performed.
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


