Pneumocystis, Jiroveci Pneumonia
Jud W. Gurney, MD, FACR
Key Facts
Terminology
Opportunistic fungal infection often affecting individuals with T-cell immunodeficiency
Imaging Findings
Ground-glass is dominant finding; opacities symmetric and diffuse with sparing of lung periphery (40%)
Mosaic attenuation pattern (30%)
Upper lobe distribution in some, may be associated with aerosolized pentamidine prophylaxis
Cysts (30%), thin-walled, usually in ground-glass opacities
Prior irradiated lung protected: PCP will develop only outside radiation ports
Extremely rare to have PCP with normal HRCT examination
Top Differential Diagnoses
Hypersensitivity Pneumonitis
Lymphocytic Interstitial Pneumonia
Diffuse Alveolar Hemorrhage
Pathology
Patients with impaired cell-mediated immunity predisposed to PCP
Organism can be found in normal lungs
Even with highly active antiretroviral therapy (HAART), PCP remains most prevalent opportunistic infection in AIDS
Clinical Issues
Nonproductive cough (75%), fever (75%), dyspnea (65%), and hypoxia
Appropriately treated PCP has very good prognosis
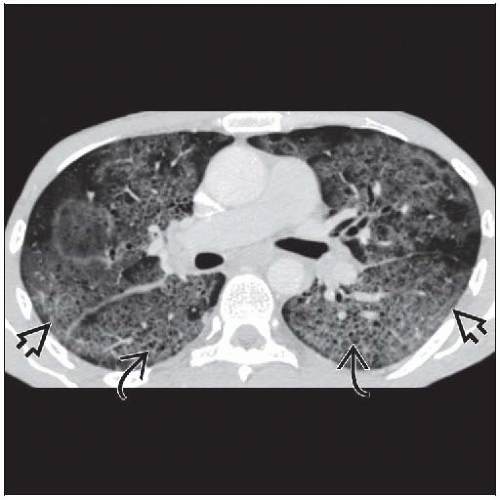 Axial CECT shows diffuse ground-glass opacities  with lobular sparing. Small holes with lobular sparing. Small holes  may represent early pneumatoceles. may represent early pneumatoceles. |
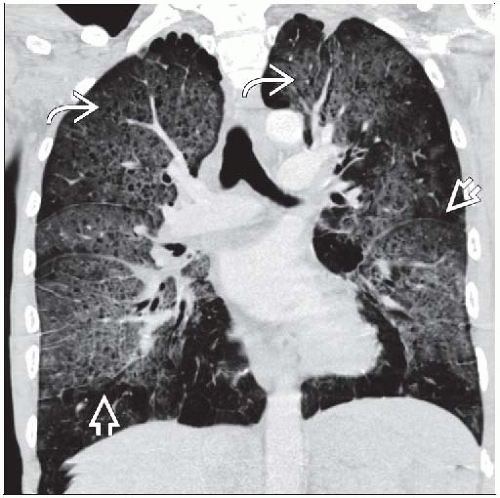 Coronal CECT reconstructions shows diffuse perihilar distribution of ground-glass opacities  and small pneumatoceles and small pneumatoceles  . . |
TERMINOLOGY
Abbreviations and Synonyms
Pneumocystis pneumonia (PCP)
Definitions
Opportunistic fungal infection often affecting individuals with T-cell immunodeficiency
2 major forms: Trophozoites and cysts
IMAGING FINDINGS
General Features
Best diagnostic clue: Diffuse symmetric ground-glass opacities in hypoxic immunocompromised patient
Patient position/location
Diffuse perihilar with peripheral sparing
Less common upper lobe predominant with cysts
Morphology: Ground-glass opacities with cysts (30%)
CT Findings
Morphology
Ground-glass is dominant finding
Diffuse infections (predominantly PCP) is most common cause of isolated diffuse ground-glass opacities
Superimposed intralobular and smooth interlobular septal thickening less common, results in “crazy-paving” pattern
Cysts (30%)
Thin-walled, usually in ground-glass opacities
Usually upper lobe distribution
Predispose to pneumothorax
With successful treatment, resolve over 5 months
Rarely described in non-AIDS PCP
Atypical patterns (5-10%) such as multiple nodules (some with cavitation), asymmetric consolidations or rarely, dominant reticular opacities
Multiple nodules (may cavitate)
Asymmetric consolidation
Reticular (interlobular and intralobular) opacities rarely dominant finding
Distribution
AIDS
Ground-glass opacities symmetric and diffuse with sparing of lung periphery 40%
Mosaic attenuation pattern 30%
Upper lobe distribution in some; may be associated with aerosolized pentamidine prophylaxis
Non-AIDS: Often spares 1 lung zone (upper, middle, lower)
Prior irradiated lung protected: PCP will develop only outside radiation ports
Other
Adenopathy uncommon (10%), short axis diameter > 1 cm
More common with other fungal or tuberculous infection
Tree-in-bud pattern not present
Consider bacterial pneumonia, aspiration, or endobronchial tuberculosis
Pleural effusion rare
In AIDS, confidant diagnosis can be made in 95%
Radiographic Findings
May be normal
Spontaneous pneumothorax in patients with AIDS = Pneumocystis pneumonia
Nuclear Medicine Findings
Historically, gallium scan used for questionable cases, now replaced by CT due to long imaging times (24 hours)
Widespread lung activity is present with PCP
Imaging Recommendations
Best imaging tool: Extremely rare to have PCP with normal HRCT examination
DIFFERENTIAL DIAGNOSIS
Hypersensitivity Pneumonitis
Antigen source identified with careful work and personal history
Onset of dyspnea and nonproductive cough tends to be more subacute or chronic
Hypoxia often more mild and fever less common
Diffuse ground-glass most common imaging manifestation
Ill-defined centrilobular nodules more common than in PCP
Air-trapping common at expiratory CT, uncommon with PCP
May also have cysts
Lymphocytic Interstitial Pneumonia
Increased frequency in AIDS, especially in children
Thin-walled cysts, ground-glass opacities, and centrilobular nodules
Lymph nodes may be enlarged, uncommon with PCP
Diffuse Alveolar Hemorrhage
Anemia common
Clinical history, tissue sampling, and laboratory investigation required to differentiate different etiologies of DAH
Diffuse or extensive bilateral ground-glass and consolidative opacities similar to PCP
Cytomegalovirus Pneumonitis
Similar predisposition (cell-mediated immunodeficiency): Most common associated infection with PCP
Bilateral diffuse ground-glass opacities most frequent finding
Centrilobular nodules (often admixed with ground-glass opacities) more common than in PCPRelated posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree



