KEY WORDS
External Sphincter. Concentric muscle group deep to the internal sphincter.
Fistula in Ano. Track that extends from the skin near the anus to the muscles surrounding the anus.
Fecal Incontinence. Involuntary leakage of fecal material through the anus.
Internal Sphincter. Ring of muscle that surrounds the anus and lies under the mucosa and submucosa.
Puborectalis Muscle. Muscle extending from the rectal wall to the pubic symphysis.
Villous Adenoma. Benign tumor of the rectal wall.
RELEVANT LABORATORY VALUES
Serum carcinoembryonic antigen (CEA). CEA is a colorectal tumor marker. The normal range is less than 2.5 ng/mL in an adult nonsmoker and less than 5.0 ng/mL in a smoker. Abnormal values are not specific for colon cancer or malignancy. CEA determination may have prognostic value for patients with colon cancer and may be used to monitor treatment, but fails to detect recurrent disease in more than 50% of patients. CEA usually returns to normal within 1 to 2 months of surgery.
The Clinical Problem
The anus and rectal wall are best imaged with a transducer in the rectum (transrectal sonography). Rectal neoplasms may be locally excised if the tumor is contained within the rectal wall. However, if the tumor extends into the perirectal fat or adjacent organs, local excision is not possible. Transrectal ultrasound has been found to be an excellent method to determine whether the tumor extends beyond the rectal wall. Because transrectal transducers extend approximately 10 to 12 cm into the rectum, tumors beyond this range cannot be examined.
When the muscles of the anus are damaged, patients experience fecal incontinence. Transrectal ultrasound can assess tears in the internal sphincter that may be the cause of fecal incontinence.
Finally, for inflammatory processes, transrectal and transvaginal ultrasound may be useful to define fistulous tracks and abscesses around the rectum.
Anatomy
RECTUM
The rectal wall consists of five alternating echogenic and echopenic layers (Fig. 23-1):
1. Transducer interface and mucosa: mildly echogenic, most superficial layer
2. Muscularis mucosa: echopenic ring deep to mucosa
3. Submucosa: brightest echogenic layer of rectal wall
4. Muscularis propria: deepest echopenic ring that is generally slightly thicker than muscularis mucosa
5. Perirectal fat: echogenic area surrounds rectal wall
Anterior to the rectum are the cervix and vagina in the female and prostate and seminal vesicles in the male.
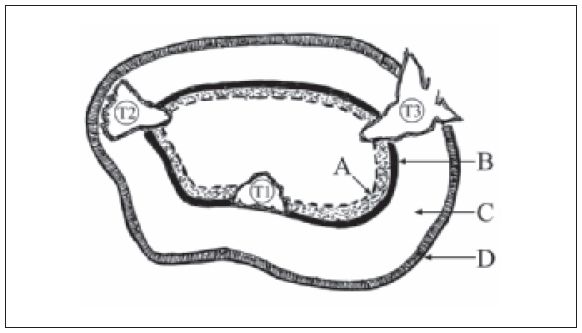
Figure 23-1. ![]() Schematic view of the rectal wall. There are four layers of the rectal wall. The mucosa/transducer interface (A) is echogenic. The muscularis mucosa (B) and muscularis propria (D) are echopenic. The submucosa (C) is the most hyperechoic layer of the wall. The tumors are classified by their location. T1 tumors are confined to the mucosa and submucosa. T2 tumors extend into the submucosa but do not invade the muscularis propria. T3 tumors breach the muscularis propria and extend into the subserosal fat.
Schematic view of the rectal wall. There are four layers of the rectal wall. The mucosa/transducer interface (A) is echogenic. The muscularis mucosa (B) and muscularis propria (D) are echopenic. The submucosa (C) is the most hyperechoic layer of the wall. The tumors are classified by their location. T1 tumors are confined to the mucosa and submucosa. T2 tumors extend into the submucosa but do not invade the muscularis propria. T3 tumors breach the muscularis propria and extend into the subserosal fat.
ANUS
The anus is dominated by the two sphincter muscles (Fig. 23-2):
1. Transducer and mucosa interface: mildly echogenic, superficial layer.
2. Internal sphincter: well-defined echopenic ring deep to the mucosa.
3. External sphincter: ill-defined area of heterogeneous echogenicity deep to the internal sphincter.
4. Puborectalis muscle: forms a sling that wraps around the anus and blends into the external sphincter approximately 2 cm from the anal margin. It attaches to the symphysis pubis.
Technique
RECTAL APPROACH
Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


